Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sixth House - Psychology of Self-Integration - Robert Glasscock - B00F07KNZ0 - EBOKDokument155 SeitenThe Sixth House - Psychology of Self-Integration - Robert Glasscock - B00F07KNZ0 - EBOKAndrew Khabaza100% (6)
- Case Taking ProformaDokument7 SeitenCase Taking ProformaDr Dushyant Kamal Dhari50% (2)
- 100 Test Aarogya 2.0:: Mrs - Gunjan MisraDokument19 Seiten100 Test Aarogya 2.0:: Mrs - Gunjan Misramomo misraNoch keine Bewertungen
- BIO 1 Course Syllabus UPDDokument3 SeitenBIO 1 Course Syllabus UPDDanielle Marie100% (1)
- Systems and RequirementsDokument3 SeitenSystems and RequirementshksbrewerNoch keine Bewertungen
- VIEW of The SS Rotating DRUM MixerDokument3 SeitenVIEW of The SS Rotating DRUM MixerhksbrewerNoch keine Bewertungen
- SS Rotating DRUM MixerDokument3 SeitenSS Rotating DRUM MixerhksbrewerNoch keine Bewertungen
- Headlines From Newspapers: 10.07.2017: 2 News ArticlesDokument3 SeitenHeadlines From Newspapers: 10.07.2017: 2 News ArticleshksbrewerNoch keine Bewertungen
- Headlines For 02Dokument1 SeiteHeadlines For 02hksbrewerNoch keine Bewertungen
- Headlines TodayDokument6 SeitenHeadlines TodayhksbrewerNoch keine Bewertungen
- Headlines Today 1Dokument2 SeitenHeadlines Today 1hksbrewerNoch keine Bewertungen
- To DoDokument1 SeiteTo DohksbrewerNoch keine Bewertungen
- Excel TipsDokument14 SeitenExcel TipshksbrewerNoch keine Bewertungen
- Images 3Dokument2 SeitenImages 3hksbrewerNoch keine Bewertungen
- Desert AnimalsDokument1 SeiteDesert AnimalshksbrewerNoch keine Bewertungen
- Third Party LetterDokument1 SeiteThird Party LetterhksbrewerNoch keine Bewertungen
- Desert PolarDokument3 SeitenDesert PolarhksbrewerNoch keine Bewertungen
- Images 2Dokument4 SeitenImages 2hksbrewerNoch keine Bewertungen
- VocaDokument1 SeiteVocahksbrewerNoch keine Bewertungen
- Back PainDokument12 SeitenBack PainhksbrewerNoch keine Bewertungen
- VocaDokument1 SeiteVocahksbrewerNoch keine Bewertungen
- Apples Oranges Lemon India 60 30 24 UZB 90 35 28 KZH 33 56 44 Iran 45 56 78Dokument1 SeiteApples Oranges Lemon India 60 30 24 UZB 90 35 28 KZH 33 56 44 Iran 45 56 78hksbrewerNoch keine Bewertungen
- TAM SAM SOM - What It Means and Why It MattersDokument2 SeitenTAM SAM SOM - What It Means and Why It MattershksbrewerNoch keine Bewertungen
- What Is A Bill of Lading 2Dokument1 SeiteWhat Is A Bill of Lading 2hksbrewerNoch keine Bewertungen
- Excel LearningDokument5 SeitenExcel LearninghksbrewerNoch keine Bewertungen
- Pivot TablesDokument7 SeitenPivot TableshksbrewerNoch keine Bewertungen
- Different Functions in ExcelDokument4 SeitenDifferent Functions in ExcelhksbrewerNoch keine Bewertungen
- Save The Indian Rupee: You Can Make A Huge Difference To The Indian Economy by Following Few Simple StepsDokument5 SeitenSave The Indian Rupee: You Can Make A Huge Difference To The Indian Economy by Following Few Simple StepshksbrewerNoch keine Bewertungen
- KabirDokument3 SeitenKabirhksbrewer100% (1)
- Bus Route Mysore CalicutDokument2 SeitenBus Route Mysore CalicuthksbrewerNoch keine Bewertungen
- Maths SyllabusDokument1 SeiteMaths SyllabushksbrewerNoch keine Bewertungen
- ImrpovementsDokument2 SeitenImrpovementshksbrewerNoch keine Bewertungen
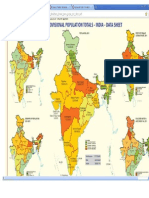
- Map of IndiaDokument1 SeiteMap of IndiahksbrewerNoch keine Bewertungen
- Hidetaka Nomura Et Al. (2015)Dokument4 SeitenHidetaka Nomura Et Al. (2015)Janardana GedeNoch keine Bewertungen
- Impaction in Dairy Animals: Ashwani KumarDokument6 SeitenImpaction in Dairy Animals: Ashwani KumarGiriNoch keine Bewertungen
- Risk Factors For CKDDokument2 SeitenRisk Factors For CKDgigolo13Noch keine Bewertungen
- Protozoa and Fungi Culturing in The LabDokument7 SeitenProtozoa and Fungi Culturing in The LabrorenNoch keine Bewertungen
- DAX2018790204 SpainDokument64 SeitenDAX2018790204 SpainHarsh BhattNoch keine Bewertungen
- Natural Medicine IODINE by Sue Visser.4810627Dokument3 SeitenNatural Medicine IODINE by Sue Visser.4810627relativelabs2075Noch keine Bewertungen
- NearfatalasthmaDokument8 SeitenNearfatalasthmaHeath HensleyNoch keine Bewertungen
- Bio Chapter 14 NotesDokument3 SeitenBio Chapter 14 NotesAvehiNoch keine Bewertungen
- Chemistry Investigatory Project 2017-18Dokument29 SeitenChemistry Investigatory Project 2017-18Ashok KumarNoch keine Bewertungen
- Evolution in Teddy Grahams MTDokument1 SeiteEvolution in Teddy Grahams MTapi-302703920Noch keine Bewertungen
- Personal Trainer Magazine ISSUE 13Dokument45 SeitenPersonal Trainer Magazine ISSUE 13Jesmin AraNoch keine Bewertungen
- Scheme of Instruction IIScDokument236 SeitenScheme of Instruction IIScRS1678Noch keine Bewertungen
- CLD FinalDokument17 SeitenCLD FinalHervis FantiniNoch keine Bewertungen
- Newport International Journal of Scientific and Experimental Sciences (Nijses) Volume 3 Issue 2 2023Dokument8 SeitenNewport International Journal of Scientific and Experimental Sciences (Nijses) Volume 3 Issue 2 2023KIU PUBLICATION AND EXTENSIONNoch keine Bewertungen
- Basal Osseointegrated Implants ClassificDokument7 SeitenBasal Osseointegrated Implants ClassificAnkur SaladaNoch keine Bewertungen
- A Biological Profile For Diagnosis and Outcome of COVID-19 PatientsDokument10 SeitenA Biological Profile For Diagnosis and Outcome of COVID-19 PatientsAristidesNoch keine Bewertungen
- Molecular Biology R - F - Weaver 5th EdDokument1 SeiteMolecular Biology R - F - Weaver 5th EdAlapan NandaNoch keine Bewertungen
- Notice: Ocean Transportation Intermediary Licenses: InterCaribbean Cargo, Inc., Et Al.Dokument2 SeitenNotice: Ocean Transportation Intermediary Licenses: InterCaribbean Cargo, Inc., Et Al.Justia.comNoch keine Bewertungen
- Pediatric DiabeticDokument9 SeitenPediatric Diabeticperla islasNoch keine Bewertungen
- Extensive Reading - AVK44CDokument42 SeitenExtensive Reading - AVK44CNinh Nhat Thao Vy K189Noch keine Bewertungen
- US Army Medical Pharmacology IDokument202 SeitenUS Army Medical Pharmacology ISpace_Hulker100% (2)
- 2018 - ICRU 83 - BaliDokument86 Seiten2018 - ICRU 83 - BalisanggamNoch keine Bewertungen
- Physiology Study Guide CH 7 Nervous System Neurons KeyDokument4 SeitenPhysiology Study Guide CH 7 Nervous System Neurons KeyJamie SamuelNoch keine Bewertungen
- Spine Magnetic Resonance Image Segmentation Using Deep Learning TechniquesDokument6 SeitenSpine Magnetic Resonance Image Segmentation Using Deep Learning TechniquesSandeep VermaNoch keine Bewertungen
- Dosage Chapter 1 PDFDokument4 SeitenDosage Chapter 1 PDFLena EmataNoch keine Bewertungen
- ASV GalileoDokument43 SeitenASV GalileoalvyandaniNoch keine Bewertungen