Das könnte Ihnen auch gefallen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- Aa 21Dokument2 SeitenAa 21drSonySpAnNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Mediva Product ListDokument8 SeitenMediva Product ListArif ParvezNoch keine Bewertungen
- Handin 1 - Cialis PPT PresentationDokument14 SeitenHandin 1 - Cialis PPT PresentationMia_NaterNoch keine Bewertungen
- Side Effects of Pregabalin DrugDokument20 SeitenSide Effects of Pregabalin DrugtulipcatcherNoch keine Bewertungen
- Semi Solids PDFDokument3 SeitenSemi Solids PDFAsif Hasan NiloyNoch keine Bewertungen
- Daftar Obat High Alert Instalasi Farmasi Rsia Mutiara BundaDokument1 SeiteDaftar Obat High Alert Instalasi Farmasi Rsia Mutiara BundaAnonymous idPPyERfBnNoch keine Bewertungen
- Joannie C. Palec Post Graduate InternDokument40 SeitenJoannie C. Palec Post Graduate InternJoannie PalecNoch keine Bewertungen
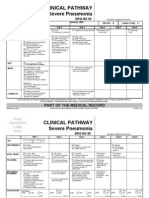
- Clinical Pathways Severe PneumoniaDokument2 SeitenClinical Pathways Severe PneumoniaaandakuNoch keine Bewertungen
- Edition, Churchill: Daftar PustakaDokument2 SeitenEdition, Churchill: Daftar Pustakairmayani jubriNoch keine Bewertungen
- Awareness of Medication-Related Fall Risk A Survey of Communitydwelling Older Adults PDFDokument7 SeitenAwareness of Medication-Related Fall Risk A Survey of Communitydwelling Older Adults PDFRenaldiPrimaSaputraNoch keine Bewertungen
- Nama Obat Jumlah Jenis Harga: Estimasi Persiapan Obat Kegiatan PramukaDokument2 SeitenNama Obat Jumlah Jenis Harga: Estimasi Persiapan Obat Kegiatan PramukaMiracle AcleNoch keine Bewertungen
- Bio Availability and Bioequivalane-LastDokument13 SeitenBio Availability and Bioequivalane-LastAhmedothman62100% (1)
- Antidote Meds in Crash Cart (Naloxone, Hydrobromide, Flumazenil)Dokument5 SeitenAntidote Meds in Crash Cart (Naloxone, Hydrobromide, Flumazenil)Still DollNoch keine Bewertungen
- Agoraphobia 1Dokument47 SeitenAgoraphobia 1We Are HanakoNoch keine Bewertungen
- The Sequenced Treatment Alternatives To Relieve DepressionDokument30 SeitenThe Sequenced Treatment Alternatives To Relieve DepressionAhmad DabbasNoch keine Bewertungen
- Buku Harian GittaDokument9 SeitenBuku Harian GittaSRI MULYANINoch keine Bewertungen
- Blueprints PsychiatryDokument466 SeitenBlueprints Psychiatrynoir100% (5)
- Rudy The Dope DealerDokument17 SeitenRudy The Dope DealerAlan Jules WebermanNoch keine Bewertungen
- 9 Ehtylcellulose Coating OPTDokument1 Seite9 Ehtylcellulose Coating OPTKumar GalipellyNoch keine Bewertungen
- Patient Group Direction (PGD) For The Administration of Local Anaesthetics and Corticosteroids BY TENDAYI MUTSOPOTSIDokument18 SeitenPatient Group Direction (PGD) For The Administration of Local Anaesthetics and Corticosteroids BY TENDAYI MUTSOPOTSIPhysiotherapy Care SpecialistsNoch keine Bewertungen
- CHRONIC RECURRENT APHTHOUS STOMATITISDokument38 SeitenCHRONIC RECURRENT APHTHOUS STOMATITISAlex DaniciNoch keine Bewertungen
- Chemotherapy DrugsDokument5 SeitenChemotherapy DrugsvmanuNoch keine Bewertungen
- California Retailers Guide To Hazardous Waste ComplianceDokument4 SeitenCalifornia Retailers Guide To Hazardous Waste ComplianceStericycle100% (1)
- Compounding and DispensingDokument9 SeitenCompounding and DispensingElida Rizki MhNoch keine Bewertungen
- CALABANGA MONITORING - OdsDokument10 SeitenCALABANGA MONITORING - Odsglecy malateNoch keine Bewertungen
- MenevitDokument6 SeitenMenevitjalutukNoch keine Bewertungen
- Merchant Shipping (Medical Stores) Regulations 1996 - First ScheduleDokument21 SeitenMerchant Shipping (Medical Stores) Regulations 1996 - First ScheduleLoka Radhakrishna NarasaiahNoch keine Bewertungen
- Lampiran 1. Sample Counting A. GudangDokument20 SeitenLampiran 1. Sample Counting A. GudangTika AndrianiNoch keine Bewertungen
- Role Play Conversations With A PharmacistDokument5 SeitenRole Play Conversations With A PharmacistIwellNoch keine Bewertungen
- AntihistaminesDokument2 SeitenAntihistaminesdeepalisharma6Noch keine Bewertungen
- Generic Name TizanidineDokument3 SeitenGeneric Name TizanidinemadamcloudnineNoch keine Bewertungen