Das könnte Ihnen auch gefallen
- Orthognatic Surgery: Mandible IDokument1 SeiteOrthognatic Surgery: Mandible IHendy NurahadiNoch keine Bewertungen
- Variations in Impacted Mandibular Permanent MolarsDokument9 SeitenVariations in Impacted Mandibular Permanent MolarsHendy NurahadiNoch keine Bewertungen
- Texture Analysis of CT Images in The Characterization of OralDokument7 SeitenTexture Analysis of CT Images in The Characterization of OralHendy NurahadiNoch keine Bewertungen
- Pps 2Dokument5 SeitenPps 2Hendy NurahadiNoch keine Bewertungen
- Palatal Abses IbnuDokument3 SeitenPalatal Abses IbnuHendy NurahadiNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- J of Cosmetic Dermatology - 2023 - Palauro - Innovation of The Protocol For The Application of Cryolipolysis Effects andDokument9 SeitenJ of Cosmetic Dermatology - 2023 - Palauro - Innovation of The Protocol For The Application of Cryolipolysis Effects andPaolaNoch keine Bewertungen
- Current issues and advances in postoperative pain managementDokument17 SeitenCurrent issues and advances in postoperative pain managementAmade DeaNoch keine Bewertungen
- 33 - Nasal Fractures PDFDokument15 Seiten33 - Nasal Fractures PDFcarlosNoch keine Bewertungen
- Research Forehead FillerDokument5 SeitenResearch Forehead FillerNavaphon ChanbangNoch keine Bewertungen
- Gifted HandsDokument8 SeitenGifted HandsMichelle Arellano67% (3)
- Apendicits NiñosDokument25 SeitenApendicits NiñosArturo SantiagoNoch keine Bewertungen
- Case Study Dr. Sisk LCA Gene Therapy MC 0005054 21NOV2022Dokument6 SeitenCase Study Dr. Sisk LCA Gene Therapy MC 0005054 21NOV2022SALAH YOUNISNoch keine Bewertungen
- Ambulatory Hysteroscopy - Creating Certainty: The Solution For Diagnostics and Treatment in An Ambulatory SettingDokument2 SeitenAmbulatory Hysteroscopy - Creating Certainty: The Solution For Diagnostics and Treatment in An Ambulatory Settingreta.rose92Noch keine Bewertungen
- Emergency Airway Management in Patients With COVID-19: A Prospective International Multicenter Cohort StudyDokument12 SeitenEmergency Airway Management in Patients With COVID-19: A Prospective International Multicenter Cohort Studyluisfernandoamaya89Noch keine Bewertungen
- Boh Luli 2019Dokument3 SeitenBoh Luli 2019Francisco ChourioNoch keine Bewertungen
- Pediatric TracheostomyDokument45 SeitenPediatric Tracheostomytsega tilahunNoch keine Bewertungen
- Tirumala Tirupati Devasthanams: TirupatiDokument3 SeitenTirumala Tirupati Devasthanams: Tirupativenkatraju.YNoch keine Bewertungen
- Causes and Management of Upper GI BleedingDokument4 SeitenCauses and Management of Upper GI BleedingRazi HaiderNoch keine Bewertungen
- Hernia: Information For PatientsDokument2 SeitenHernia: Information For Patientsrianrifaldi123_98497Noch keine Bewertungen
- 153Dokument8 Seiten153Hélder MouraNoch keine Bewertungen
- Semiology of Insular Lobe SeizuresDokument6 SeitenSemiology of Insular Lobe SeizuresViviana Torres BallesterosNoch keine Bewertungen
- Graston TechniqueDokument8 SeitenGraston TechniqueSvetlana PolyakovaNoch keine Bewertungen
- Unintentional Trauma During Gynaecological Surgery: I. Z. MackenzieDokument8 SeitenUnintentional Trauma During Gynaecological Surgery: I. Z. Mackenziemuhammadnurul asmiNoch keine Bewertungen
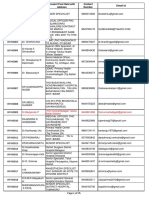
- Contact details of medical officers in KarnatakaDokument25 SeitenContact details of medical officers in KarnatakaShweta jain100% (1)
- Classification of Mandibular Condylar Fractures: David B. Powers, MD, DMD, FRCS (Ed)Dokument10 SeitenClassification of Mandibular Condylar Fractures: David B. Powers, MD, DMD, FRCS (Ed)Mashood AhmedNoch keine Bewertungen
- Irish Tatler Emface 1674483099 OriginalDokument1 SeiteIrish Tatler Emface 1674483099 OriginalFelicia BuenoNoch keine Bewertungen
- Syntax Score Calculation SimulationDokument66 SeitenSyntax Score Calculation SimulationTahari Bargas PrakosoNoch keine Bewertungen
- Advances in Facial Rejuvenation Botox, HA Dermal Fillers, & Combination TherapyDokument26 SeitenAdvances in Facial Rejuvenation Botox, HA Dermal Fillers, & Combination Therapybluestes100% (1)
- Pterygium Pinguecula Post-Op GuideDokument4 SeitenPterygium Pinguecula Post-Op GuideBrandon ChienNoch keine Bewertungen
- Anatomical Shoulder Fracture System Surgical Technique PDFDokument24 SeitenAnatomical Shoulder Fracture System Surgical Technique PDFAdrian TudorNoch keine Bewertungen
- SERVO-Air Presentation Indonesia Rev SlideDokument32 SeitenSERVO-Air Presentation Indonesia Rev SlideSamsulNoch keine Bewertungen
- Total Shoulder Arthroplasty, An Overview, Indicatins and Prosthetic OptionsDokument4 SeitenTotal Shoulder Arthroplasty, An Overview, Indicatins and Prosthetic OptionsYafiahnaf FirdausNoch keine Bewertungen
- Removable Partial Denture Occlusion: John R. Ivanhoe, DDS, Kevin D. Plummer, DDSDokument17 SeitenRemovable Partial Denture Occlusion: John R. Ivanhoe, DDS, Kevin D. Plummer, DDSAna MaríaNoch keine Bewertungen
- What Happens After The Cystoscopy ProcedureDokument2 SeitenWhat Happens After The Cystoscopy ProcedureStepyn SalvadorNoch keine Bewertungen
- Female Urinary Catheter Insertion GuideDokument9 SeitenFemale Urinary Catheter Insertion GuideVinz Khyl G. CastillonNoch keine Bewertungen