Original Research
Annals of Internal Medicine
Hepatitis B Virus in the United States: Infection, Exposure, and
Immunity Rates in a Nationally Representative Survey
George N. Ioannou, BMBCh, MS
Background: Up-to-date estimates of the prevalence of hepatitis B
virus (HBV) infection, exposure, and immunity are necessary to
assess the effectiveness of ongoing programs aimed at preventing
HBV transmission.
Objective: To determine the prevalence and associations of chronic
HBV infection, past exposure, and immunity in the United States
from 1999 to 2008.
Design: Nationally representative, cross-sectional household survey.
Setting: U.S. civilian, noninstitutionalized population.
Participants: 39 787 participants in the National Health and Nutrition Examination Survey (1999 to 2008) aged 2 years or older.
Measurements: Chronic HBV infection was defined by presence of
serum HBV surface antigen and past exposure by serum antibody
to hepatitis B core antigen among persons aged 6 years or older.
Infant immunity was defined by presence of serum antibody to
hepatitis B surface antigen among children aged 2 years.
approximately 704 000 persons nationwide), and 4.6% (CI, 4.1%
to 5.0%) had been exposed to HBV (approximately 11 993 000
persons). These estimates are lower (P 0.001) than estimates of
HBV infection (0.42%) and exposure (5.1%) in the United States
reported from 1988 to 1994. Infection and past exposure were
very uncommon among persons aged 6 to 19 years. Children aged
2 years have high rates of immunity (68.6% [CI, 64.1% to
73.2%]). Adults, including those at high risk for infection, have
much lower rates of immunity.
Limitations: Incarcerated and homeless persons were not sampled.
Categorization of race or ethnicity did not identify high-risk groups,
such as persons of Asian and Pacific Islander descent.
Conclusion: A cohort of children and adolescents is growing up in
the United States with high rates of immunity against HBV and
very low rates of infection. Vaccination of high-risk adults should
continue to be emphasized.
Primary Funding Source: The Veterans Affairs Research Enhancement Award Program.
Results: Among persons aged 6 years or older, 0.27% (95% CI,
0.20% to 0.34%) had chronic HBV infection (corresponding to
Ann Intern Med. 2011;154:319-328.
For author affiliation, see end of text.
unclear whether the prevalence of HBV infection in the
United States has decreased in recent years.
Immunization is by far the single most effective measure at preventing HBV transmission. The Advisory Committee on Immunization Practices has recommended routine vaccination of all infants in the United States
regardless of the mothers hepatitis B status since 1991 (2).
Indeed, 92.4% to 93.5% of children aged 19 to 35 months
were reported by their vaccination providers to have received all 3 doses of HBV vaccination in the United States
from 2004 to 2009 (3, 4). However, it remains unclear
what proportion of infants have antibodies against HBV
surface antigen (anti-HBs) as a result of effective vaccination in the United States and what proportion of older
children and adults have persistence of serum anti-HBs,
levels of which are known to decline and become undetectable in a variable proportion with the passage of time after
he World Health Organization estimates that at least 2
billion persons have been infected with hepatitis B virus (HBV) worldwide, with more than 378 million persons
being chronic carriers (6% of the world population). Hepatitis B virus infection is the most important cause of liver
disease in the world, causing acute hepatitis, chronic liver
disease, cirrhosis, and hepatocellular carcinoma.
The prevalence of HBV in the United States is lower
than in endemic areas of the world but is still substantial.
Using data from the Third National Health and Nutrition
Examination Survey (NHANES III), conducted from
1988 to 1994, it was estimated that 5.1% of the U.S.
population had been exposed to HBV, as evidenced by
presence in serum of antibodies to hepatitis B core antigen
(anti-HBc), and 0.42% had chronic HBV infection, as evidenced by serum HBV surface antigen (HBsAg) (1).
The incidence of new HBV infections might be expected to have decreased in recent years as a result of more
widespread vaccination in children, as well as improvements in needle-using practices and effective exclusion of
HBV-infected persons from blood donation. In addition,
many antiviral agents that effectively suppress viral replication have become available, although they lead to elimination of HBsAg only rarely. In contrast, persons of Asian
and Pacific Islander descent, racial groups with a particularly high prevalence of HBV infection, constitute an increasing proportion of the U.S. population. Therefore, it is
www.annals.org
www.annals.org
See also:
Print
Editors Notes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 320
Web-Only
Appendix
Appendix Table
Conversion of graphics into slides
1 March 2011 Annals of Internal Medicine Volume 154 Number 5 319
Original Research
Hepatitis B Virus in the United States: Infection, Exposure and Immunity Rates
A national population-based survey showed that increased
use of HBV vaccine in pediatric settings over the past decade has resulted in a cohort of children and adolescents
with a very low prevalence of HBV infection and high
rates of immunity that suggest significant protection
against future infection. In contrast, adults, including those
at high risk for HBV infection, continue to have low rates
of immunity against this virus.
NHANES comprised a stratified, multistage probability sample of the civilian, noninstitutionalized U.S. population of all 50 states and the District of Columbia. Extensive efforts were made to ensure participation. All
participants were reimbursed for their time, transportation,
and childcare expenses, if necessary. Participants were initially interviewed in person at home and then invited to
attend a mobile examination center for examinations,
blood tests, and additional interviews.
Participants aged 2 years or older (n 47 484) were
eligible for anti-HBs testing, of whom 39 787 gave a suitable blood sample (final response rate for testing was
83.8%). Only participants aged 6 years or older (n 42
773) were eligible for anti-HBc and HBsAg testing, of
whom 37 259 (87%) were tested. Persons with or without
available HBV serologic testing did not substantially differ
with respect to major risk factors for HBV infection (age,
sex, and race or ethnicity).
Caution
Laboratory Methods
Some populations at high risk for HBV infection were
excluded from or underrepresented in this survey.
Collected blood specimens were processed, stored, and
shipped to the Division of Viral Hepatitis, National Center
for Infectious Diseases (Atlanta, Georgia). Enzyme-linked
immunoassays were used to measure HBsAg (AUSZYME,
Abbott Laboratories, Chicago, Illinois), anti-HBs (AUSAB,
Abbott Laboratories), and anti-HBc (Ortho HBc ELISA
Tests System, Ortho Clinical Diagnostics, Rochester, New
York). Specimens that tested nonreactive were considered
negative and were not tested further. Specimens considered
reactive initially were repeat-tested in duplicate. If neither
of the repeated tests was reactive, the specimen was considered negative. If the specimen was reactive in either of
the repeated tests, the sample was considered repeatedly
reactive. Results were expressed qualitatively as positive or
negative for anti-HBc, anti-HBs, and HBsAg. No quantitative results were determined. In the case of anti-HBs, a
positive result has a quantitative interpretation of greater
than 10 IU/L (13).
Context
Hepatitis B virus (HBV) infection is an important cause of
morbidity and mortality in the United States. Population
demographic characteristics, the use of HBV vaccine, and
behaviors that lead to exposure to HBV have been changing over the past 2 decades. Current estimates of HBV
infection and immunity are needed to appropriately target
prevention and treatment efforts.
Contribution
Implication
Real progress has been made in protecting children and
adolescents in the United States from HBV infection.
Adults remain an important population for targeted
immunization efforts.
The Editors
vaccination (511). Although disappearance of anti-HBs
does not necessarily indicate loss of protection (12), presence of anti-HBs has been shown to be a correlate of immunity, both against infection and persistence, and is the
easiest way to demonstrate existing protection.
The aim of this project was to determine up-to-date
estimates of infection, exposure, and immunity rates for
HBV in the United States population by using data from
the NHANES studies conducted from 1999 to 2008.
METHODS
Study Design
NHANES consists of a series of cross-sectional studies
designed to estimate the number and percentage of persons
in the U.S. population and designated subgroups with selected diseases and risk factors. Since 1999, NHANES
studies have been released every 2 years and are designed
such that multiple 2-year periods can be combined to yield
more accurate estimates of uncommon conditions. Because
of the relatively small number of HBV-infected persons,
data from 5 consecutive 2-year periods (1999 to 2008)
were combined. The NHANES data sets, related documentation, and analytic guidelines are made available by
the National Center for Health Statistics (www.cdc.gov
/nchs/nhanes.htm).
320 1 March 2011 Annals of Internal Medicine Volume 154 Number 5
Definition of HBV Status: Chronic Infection, Exposure,
and Vaccination-Induced Immunity
Chronic infection was defined by a positive serum
HBsAg result. Exposure to HBV was defined by a positive
anti-HBc result, which signifies either past or present infection. Vaccination-induced immunity was defined as a
positive anti-HBs result in the absence of anti-HBc, in
order to identify persons in whom anti-HBs was induced
by vaccination rather than exposure to the virus, among
persons aged 6 years or older. Among children aged 2 to 5
years, vaccination-induced immunity was defined only by a
positive anti-HBs result because anti-HBc was not ascertained in that age group. This is a reasonable approximation because exposure to HBV in that age group is very low
in the United States (0.5%).
Vaccination-induced immunity, as defined herein, underestimates receipt of previous vaccination, particularly
among adults, because anti-HBs levels decline with time
www.annals.org
Hepatitis B Virus in the United States: Infection, Exposure and Immunity Rates
and may become negative in a large proportion of previously vaccinated persons (511). However, among children
aged 2 years, the presence of anti-HBs probably reflects
effective infant hepatitis B vaccination with reasonable accuracy: Children aged 2 years should have completed their
recommended hepatitis B vaccination series but should not
have experienced any substantial decline in anti-HBs levels.
Hence, prevalence of anti-HBs is reported separately
among children aged 2, 3, 4, and 5 years.
Absence of vaccination-induced immunity, as defined
herein, does not necessarily indicate absence of protection
against HBV infection because persistence of immunologic
memory can still be detected in vitro in peripheral blood
lymphocytes from persons whose anti-HBs has become undetectable in vivo (14). However, detecting the presence of
anti-HBs is the easiest way to demonstrate existing immune protection in a population, and rates of anti-HBs in
adults may inform future discussions on whether booster
vaccinations are required in adults.
Statistical Analysis
Stata/SE software, version 11 (StataCorp, College Station, Texas) was used for all analyses. NHANES used a
complex, multistage sampling design, including oversampling for certain demographic groups (low-income persons,
adolescents aged 12 to 19 years, persons aged 60 years or
older, and black and Mexican persons). Weights are pro-
Original Research
vided to account for oversampling as well as survey nonresponse and a poststratification adjustment to match the
year 2000 U.S. census. The survey commands of Stata
were used to account for both the sampling and the
weighting processes, such that the results are representative
of the U.S. population. The variables used to denote the
primary sampling units and strata were sdmvpsu and sdmvstra, respectively. Appropriate weights were calculated for
the 10-year period by multiplying 4/10 times the 4-year
weight provided by the NHANES for 1999 to 2002 (4/
10 wtmec4yr) and 2/10 times the 2-year weights provided for each period 2003 to 2004, 2005 to 2006, and
2007 to 2008 (2/10 wtmec2yr) (15).
The prevalence and 95% CIs of serologic markers of
HBV in the United States were calculated for the entire
population and among subgroups defined by selected risk
factors for HBV by using the svy:proportion command in
Stata. Prevalence was multiplied by the total civilian, noninstitutionalized population in the United States averaged
across the NHANES studies from 1999 to 2008 (www.cdc
.gov/nchs/nhanes/response_rates_CPS.htm) for persons
aged 6 years or older (about 262 611 444) to estimate the
number of persons. Univariate and multivariate logistic regression were used to determine the unadjusted and adjusted odds ratios and 95% CIs of selected predictors of
infection, exposure, or immunity, by using the svy:logit
Table 1. Prevalence and Predictors of Chronic Hepatitis B Virus Infection (Positive HBsAg) Among Persons Aged 6 Years or Older
in the United States, 1999 to 2008
Variable
Participants Tested, n
All participants
37 259
0.27 (0.200.34)
NA
Sex
Female
Male
19 033
18 226
0.17 (0.090.24)
0.38 (0.250.50)
1
2.27 (1.313.96)
5833
5931
6508
3956
3900
3148
3583
4400
0.03 (0.000.06)
0.02 (0.000.04)
0.25 (0.090.42)
0.31 (0.150.47)
0.33 (0.160.50)
0.57 (0.330.81)
0.19 (0.030.35)
0.20 (0.050.34)
1
0.63 (0.142.8)
9.6 (2.537)
11.6 (2.947)
12.5 (4.039)
21.5 (6.472)
7.1 (1.241)
7.4 (1.831)
Age
612 y
1317 y
1829 y
3039 y
4049 y
5059 y
6069 y
70 y
Prevalence of HBsAg
(95% CI), %
Unadjusted OR
(95% CI)
Race or ethnicity
Non-Hispanic white
Non-Hispanic black
Hispanic*
Other race
15 259
8850
11 670
1480
0.11 (0.060.15)
0.73 (0.41.0)
0.05 (0.0030.11)
1.97 (1.02.9)
1
6.9 (3.713.1)
0.52 (0.21.5)
19.0 (10.235.5)
Birthplace
United States
Mexico
Elsewhere (white, black, or Hispanic)
Elsewhere and other race
30 181
4056
2419
577
0.17 (0.110.22)
0.026 (0.00.0007)
0.59 (0.270.91)
3.28 (1.415.14)
1
0.16 (0.030.82)
3.6 (1.96.6)
20.4 (10.340.6)
HBsAg hepatitis B surface antigen; NA not applicable; OR odds ratio.
* Includes Mexican Americans and other Hispanic persons.
www.annals.org
1 March 2011 Annals of Internal Medicine Volume 154 Number 5 321
Original Research
Hepatitis B Virus in the United States: Infection, Exposure and Immunity Rates
Table 2. Prevalence and Predictors of Exposure to Hepatitis B Virus (Positive Anti-HBc) Among Persons Aged 6 Years or Older in
the United States, 1999 to 2008
Characteristic
Participants
Tested, n
Aged >6 y*
Aged 2059 y
Aged 2049 y
All participants
37 259
4.6 (4.15.0)
NA
NA
NA
NA
Sex
Female
Male
19 033
18 226
3.9 (3.44.4)
5.3 (4.75.9)
1
1.39 (1.21.6)
1
1.62 (1.41.9)
1
1.36 (1.041.8)
1
1.44 (1.072.0)
0.4 (0.060.8)
0.5 (0.30.7)
2.2 (1.62.8)
4.0 (3.34.7)
6.5 (5.57.5)
7.9 (6.79.1)
6.1 (5.07.3)
7.6 (6.39.0)
1
1.07 (0.42.8)
5.1 (2.112.5)
9.4 (2.823)
15.6 (6.537)
19.4 (7.948)
14.7 (6.036)
18.7 (7.646)
1
1.10 (0.43.1)
4.5 (1.712)
9.2 (3.524)
18.5 (7.248)
24.4 (9.265)
18.9 (7.249)
26.4 (1969)
NA
NA
1
2.3 (1.53.6)
5.0 (3.37.4)
6.4 (4.110.0)
NA
NA
NA
NA
1
1.8 (1.12.9)
3.5 (2.25.5)
NA
NA
NA
Age
612 y
1317 y
1829 y
3039 y
4049 y
5059 y
6069 y
70 y
5833
5931
6508
3956
3900
3148
3583
4400
Prevalence of
Anti-HBc,
(95% CI), %
Unadjusted OR
(95% CI)
Adjusted OR (95% CI)
Race or ethnicity
Non-Hispanic white
Non-Hispanic black
Hispanic
Other race
15 259
8850
11 670
1480
2.8 (2.53.1)
10.4 (9.411.4)
3.5 (2.74.3)
17.6 (14.820.4)
1
4.02 (3.54.6)
1.24 (0.971.6)
7.37 (69.1)
1
4.48 (3.95.2)
1.04 (0.81.4)
2.89 (1.84.6)
1
4.12 (3.25.3)
1.11 (0.71.7)
2.95 (1.55.7)
1
3.27 (2.44.5)
0.75 (0.41.3)
3.54 (1.58.2)
Birthplace
United States
Mexico
Elsewhere (white, black, or Hispanic)
Elsewhere and other race
30 181
4056
2419
577
3.4 (3.03.7)
2.4 (1.73.1)
11.0 (9.113.0)
31.3 (26.536.1)
1
0.71 (0.530.95)
3.57 (2.94.4)
13.1 (10.316.8)
1
0.86 (0.61.3)
3.30 (2.64.2)
6.72 (3.911.6)
1
0.75 (0.41.3)
3.55 (2.45.2)
8.21 (3.618.6)
1
1.21 (0.62.3)
5.0 (3.27.9)
7.0 (2.618.5)
Family income
2 times poverty threshold
11.9 times poverty threshold
Below poverty threshold
16 993
9197
8328
3.6 (3.24.0)
6.2 (5.47.0)
5.7 (4.76.7)
1
1.79 (1.52.1)
1.63 (1.12.0)
1
1.93 (1.62.3)
1.93 (1.62.4)
1
1.98 (1.52.6)
1.69 (1.32.3)
1
1.91 (1.32.7)
1.39 (0.962.0)
Education (participants aged >20 y)
12 y
12 y
7191
15 950
8.7 (7.69.8)
4.8 (4.35.3)
1
0.53 (0.470.60)
NA
NA
1
0.82 (0.61.1)
1
0.92 (0.71.3)
Marital status (participants aged >18 y)
Married
Widowed
Divorced
Separated
Never married
Living with partner
12 713
2159
2142
747
5412
1588
4.7 (4.05.3)
7.5 (6.18.9)
7.7 (6.29.1)
8.6 (6.410.8)
4.8 (3.95.6)
7.3 (5.68.9)
1
1.65 (1.322.1)
1.70 (1.42.1)
1.91 (1.42.6)
0.80 (0.670.95)
1.60 (1.22.1)
NA
NA
NA
NA
NA
NA
1
0.68 (0.31.8)
1.67 (1.12.5)
1.43 (0.92.2)
2.18 (1.63.0)
2.65 (1.83.8)
1
1.12 (0.43.5)
1.91 (1.32.9)
1.78 (1.12.9)
2.06 (1.43.1)
2.57 (1.64.0)
9710
3205
6.0 (5.26.8)
7.0 (6.17.9)
1
1.18 (0.991.4)
NA
NA
1
1.35 (1.0051.8)
1
1.07 (0.61.8)
Blood transfusion
No
Yes, 1992present
Yes, 19721991
33 623
848
1123
4.3 (3.84.7)
5.8 (3.58.2)
6.3 (4.87.8)
1
1.39 (0.92.1)
1.51 (1.21.9)
NA
NA
NA
1
0.86 (0.32.2)
1.30 (0.72.4)
1
0.49 (0.30.7)
0.99 (0.42.3)
Lifetime street drug use except marijuana
(participants aged 2059 y)
No
Noninjection drug use
Injection drug use
11 000
2485
302
4.0 (3.54.4)
5.1 (4.16.0)
27.3 (20.833.8)
1
1.29 (1.051.6)
9.1 (6.412.9)
NA
NA
NA
1
1.41 (1.071.9)
1.30 (0.72.4)
1
1.18 (0.81.7)
1.86 (0.94.0)
4.3 (3.35.3)
3.5 (3.04.1)
1
0.82 (0.61.1)
NA
NA
1
0.67 (0.50.99)
1
0.49 (0.30.7)
Served in the U.S. armed forces
No
Yes
Lifetime number of sexual partners
(participants aged 2059 y)
01
29
2134
6462
322 1 March 2011 Annals of Internal Medicine Volume 154 Number 5
www.annals.org
Hepatitis B Virus in the United States: Infection, Exposure and Immunity Rates
Original Research
Table 2Continued
Characteristic
Prevalence of
Anti-HBc,
(95% CI), %
Unadjusted OR
(95% CI)
Aged >6 y*
Aged 2059 y
Aged 2049 y
2087
1579
601
3.8 (2.94.7)
6.4 (5.07.8)
15.5 (11.919.1)
0.88 (0.61.3)
1.52 (1.12.1)
4.1 (2.85.9)
NA
NA
NA
0.58 (0.40.92)
0.92 (0.61.4)
1.82 (1.0093.3)
0.47 (0.30.8)
0.58 (0.40.9)
1.20 (0.62.5)
Antibody to hepatitis C virus
(participants aged >6 y)**
Negative
Positive
36 794
465
4.1 (3.64.5)
38.5 (32.644.4)
1
14.8 (11.219.6)
NA
NA
NA
NA
1
9.3 (4.917.6)
Antibody to HIV type 1 (participants
aged 1849 y)
Negative
Positive
11 841
73
3.9 (3.4-4.4)
50.9 (37.9-64.0)
1
25.5 (14.7-44.1)
NA
NA
NA
NA
1
19.3 (8.1-46.3)
1
3.26 (2.74.0)
NA
NA
NA
NA
1
1.87 (1.32.6)
1019
2049
50
Antibody to herpes simplex virus type 2
(participants aged 1849 y)
Negative
Positive
Participants
Tested, n
9105
2709
3.0 (2.53.5)
9.1 (7.810.5)
Adjusted OR (95% CI)
anti-HBc antibody against hepatitis B core antigen; NA not applicable; OR odds ratio.
* Adjusted for sex, race or ethnicity, age, family income, and birthplace.
Adjusted for sex, race or ethnicity, age, family income, birthplace, educational attainment, marital status, service in the U.S. armed forces, blood transfusion, lifetime street
drug use, and lifetime number of sexual partners.
Adjusted for all characteristics in the previous 2 footnotes in addition to hepatitis C virus, HIV, and herpes simplex virus 2 status.
Category includes ages 20 to 29 y for the adjusted ORs limited to persons aged 20 y.
Includes Mexican Americans and other Hispanic persons.
Only data for men aged 17 y are presented in the univariate analyses.
** Antibody to hepatitis C virus confirmed by recombinant immunoblot assay.
command in Stata. These predictors, listed in Tables 1 to
3, were determined a priori on the basis of factors known
or suspected to be associated with HBV infection, exposure, or immunity.
Estimates of the prevalence of HBV exposure and infection from NHANES 1999 to 2008 were compared with
estimates from NHANES III (1988 to 1994), which are
published elsewhere (1), by using a t statistic as described
by Korn and Graubard (16) after direct standardization of
prevalence estimates from both studies to the age and sex
distribution of the 2000 U.S. census population (17).
Role of the Funding Source
The Veterans Affairs Research Enhancement Award
Program funded the study. The funding source had no role
in the study design, conduct, interpretation of results, or in
the decision to submit the manuscript for publication.
RESULTS
Among persons aged 6 years or older, 0.27% (95% CI,
0.20% to 0.34%) had chronic HBV infection (about
704 000 persons), 4.6% (CI, 4.1% to 5.0%) had been
exposed to HBV (about 11 993 000 persons), and 22.6%
(CI, 21.8% to 23.4%) tested positive for serum anti-HBs
without anti-HBc as a result of previous vaccination
against HBV (about 59 297 000 persons). These estimates
from 1999 to 2008 were significantly lower (P 0.001)
than previous estimates for infection (0.42% [CI, 0.32%
to 0.55%]) and exposure (5.1% [CI, 4.4% to 5.8%]) in
www.annals.org
the United States published from 1988 to 1994
(NHANES III data), after additional age- and sexstandardized estimates were obtained from both periods
using U.S. census population from 2000 for comparability
(standardized estimates are shown in the Appendix, available at www.annals.org).
The prevalence of chronic HBV infection was very low
in children and adolescents aged 6 to 12 years (0.03%) and
13 to 17 years (0.02%). Prevalence increased with age,
peaking in the 50- to 59-year age group (0.57%), and
decreased in the 60- to 69-year age group (0.19%) and
among persons aged 70 years or older (0.20%) (Table 1).
Hepatitis B virus infection was more common in men
(0.38%) than in women (0.17%). Hispanic persons had
the lowest prevalence (0.05%), followed by non-Hispanic
white persons (0.11%); black persons (0.73%); and persons of other racial or ethnic groups (1.97%), most of
whom would be expected to be of Asian race or ethnicity.
The prevalence among persons born in the United States
(0.17%) or Mexico (0.026%) was much lower than the
prevalence among persons born elsewhere (0.59% if they
were white, black, or Hispanic and 3.28% if they were of
other race or ethnicity).
Exposure to HBV (Table 2) was more common in
men (5.3%) than in women (3.9%) and in non-Hispanic
black persons (10.4%) and persons of other race or ethnicity (17.6%) than in non-Hispanic white persons (2.8%)
and Hispanic persons (3.5%). Persons born outside the
1 March 2011 Annals of Internal Medicine Volume 154 Number 5 323
Original Research
Hepatitis B Virus in the United States: Infection, Exposure and Immunity Rates
Table 3. Prevalence and Predictors of the Presence of Anti-HBs but Not Anti-HBc Among Persons Aged 6 Years or Older in the
United States, 1999 to 2008
Characteristic
Participants
Tested, n
Prevalence of
Positive Anti-HBs
and Negative
Anti-HBc
(95% CI), %
Unadjusted OR
(95% CI)
Adjusted OR (95% CI)
Aged >6 y*
Aged 2059 y
Aged 2049 y
All participants
37 259
22.6 (21.823.4)
NA
NA
NA
NA
Sex
Female
Male
19 033
18 226
24.1 (23.025.2)
21.0 (20.221.8)
1
0.84 (0.790.89)
1
0.73 (0.70.8)
1
0.61 (0.50.7)
1
0.56 (0.50.7)
5833
5931
6508
3956
3900
3148
3583
4400
52.3 (49.954.7)
62.4 (59.165.6)
32.2 (30.234.1)
15.7 (14.217.2)
12.1 (10.813.5)
11.2 (10.012.5)
7.2 (6.18.3)
3.7 (2.94.5)
1
1.5 (1.31.7)
0.43 (0.40.5)
0.17 (0.10.2)
0.13 (0.110.15)
0.12 (0.100.13)
0.07 (0.060.08)
0.04 (0.030.05)
1
1.5 (1.31.7)
0.43 (0.40.5)
0.17 (0.10.2)
0.12 (0.100.14)
0.11 (0.090.12)
0.07 (0.050.08)
0.03 (0.0250.04)
NA
NA
1
0.53 (0.450.63)
0.38 (0.310.45)
0.33 (0.270.40)
NA
NA
NA
NA
1
0.56 (0.50.7)
0.40 (0.30.5)
NA
NA
NA
Race or ethnicity
Non-Hispanic white
Non-Hispanic black
Hispanic
Other race
15 259
8850
11 670
1480
21.5 (20.522.4)
24.2 (23.025.5)
24.6 (23.126.1)
28.4 (24.831.9)
1
1.17 (1.11.3)
1.20 (1.11.3)
1.45 (1.21.7)
1
0.91 (0.81.0)
1.0 (0.91.1)
1.17 (0.91.5)
1
0.86 (0.71.0)
0.92 (0.71.2)
1.48 (1.02.1)
1
0.89 (0.71.1)
0.90 (0.71.2)
1.53 (1.02.3)
Birthplace
United States
Mexico
Elsewhere (white, black, or Hispanic)
Elsewhere and other race
30 181
4056
2419
577
23.4 (22.524.3)
14.0 (12.115.9)
17.7 (15.519.9)
23.2 (18.727.7)
1
0.53 (0.460.62)
0.70 (0.590.83)
0.99 (0.771.27)
1
0.55 (0.50.7)
0.91 (0.81.1)
1.18 (0.81.6)
1
0.58 (0.40.8)
0.86 (0.61.1)
0.83 (0.51.3)
1
0.53 (0.40.8)
0.80 (0.61.1)
0.78 (0.41.4)
Family income
2 times poverty threshold
11.9 times poverty threshold
Below poverty threshold
16 993
9197
8328
22.6 (21.623.5)
21.7 (20.323.1)
26.1 (24.228.0)
1
0.95 (0.91.05)
1.21 (1.11.3)
1
0.80 (0.70.9)
0.81 (0.70.9)
1
0.81 (0.660.99)
0.78 (0.630.97)
1
0.84 (0.71.05)
0.81 (0.61.03)
Education (participants aged >20 y)
12 y
12 y
7191
15 950
7.7 (6.78.7)
15.6 (14.816.4)
1
2.21 (1.922.55)
NA
NA
1
1.75 (1.42.1)
1
1.58 (1.32.0)
Marital status (participants aged >18 y)
Married
Widowed
Divorced
Separated
Never married
Living with partner
12 713
2159
2142
747
5412
1588
12.6 (11.713.5)
5.6 (3.97.3)
11.5 (9.613.5)
11.9 (8.715.2)
27.3 (25.529.1)
18.4 (15.721.0)
1
0.42 (0.300.57)
0.90 (0.741.10)
0.94 (0.681.29)
3.88 (3.54.3)
1.57 (1.311.89)
NA
NA
NA
NA
NA
NA
1
1.09 (0.62.1)
0.87 (0.71.1)
0.83 (0.51.3)
1.42 (1.21.7)
1.08 (0.91.3)
1
0.75 (0.22.3)
0.71 (0.50.99)
0.83 (0.51.3)
1.45 (1.21.8)
1.11 (0.91.4)
9710
3205
15.6 (14.516.6)
9.2 (7.810.5)
1
0.55 (0.460.66)
NA
NA
1
1.31 (1.001.7)
1
1.60 (1.22.2)
Blood transfusion
No
Yes, 1992present
Yes, 19721991
33 623
848
1123
24.0 (23.124.8)
10.0 (7.512.4)
12.0 (10.114.0)
1
0.35 (0.270.46)
0.43 (0.360.53)
NA
NA
NA
1
0.95 (0.61.5)
1.10 (0.71.6)
1
0.99 (0.61.7)
1.28 (0.82.0)
Lifetime street drug use except marijuana
(participants aged 2059 y)
No
Noninjection drug use
Injection drug use
11 000
2485
302
17.8 (16.8-18.8)
13.7 (11.715.7)
14.7 (9.220.1)
1
0.73 (0.620.87)
0.79 (0.511.23)
NA
NA
NA
1
0.77 (0.60.9)
1.04 (0.61.7)
1
0.76 (0.60.9)
1.14 (0.62.1)
Age
612 y
1317 y
1829 y
3039 y
4049 y
5059 y
6069 y
70 y
Served in the U.S. armed forces
No
Yes
324 1 March 2011 Annals of Internal Medicine Volume 154 Number 5
www.annals.org
Hepatitis B Virus in the United States: Infection, Exposure and Immunity Rates
Original Research
Table 3Continued
Characteristic
Prevalence of
Positive Anti-HBs
and Negative
Anti-HBc
(95% CI), %
Unadjusted OR
(95% CI)
2134
6462
2087
1579
601
17.9 (15.620.2)
17.9 (16.719.2)
17.8 (15.819.8)
12.7 (10.914.4)
12.7 (9.915.4)
Antibody to hepatitis C virus
(participants aged >6 y)**
Negative
Positive
36 794
465
Antibody to HIV type 1 (participants
aged 1849 y)
Negative
Positive
Lifetime number of sexual partners
(participants aged 2059 y)
01
29
1019
2049
50
Antibody to herpes simplex virus type 2
(participants aged 1849 y)
Negative
Positive
Participants
Tested, n
Adjusted OR (95% CI)
Aged >6 y*
Aged 2059 y
Aged 2049 y
1
1.0 (0.851.18)
0.99 (0.831.18)
0.66 (0.540.82)
0.67 (0.510.87)
NA
NA
NA
NA
NA
1
0.98 (0.81.2)
1.03 (0.81.3)
0.77 (0.61.0)
0.88 (0.61.2)
1
0.98 (0.81.2)
1.07 (0.81.4)
0.75 (0.51.03)
0.81 (0.61.2)
22.8 (22.023.6)
7.7 (5.210.2)
1
0.28 (0.200.40)
NA
NA
NA
NA
1
0.66 (0.41.3)
11 841
73
20.3 (19.221.3)
11.5 (3.319.6)
1
0.51 (0.221.15)
NA
NA
NA
NA
1
0.63 (0.22.1)
9105
2709
21.7 (20.522.9)
14.3 (12.416.3)
1
0.60 (0.510.71)
NA
NA
NA
NA
1
0.79 (0.60.99)
anti-HBc antibody against hepatitis B core antigen; anti-HBs antibody against hepatitis B surface antigen; NA not applicable; OR odds ratio.
* Adjusted for sex, race or ethnicity, age, family income, and birthplace.
Adjusted for sex, race or ethnicity, age, family income, birthplace, educational attainment, marital status, service in the U.S. armed forces, blood transfusion, lifetime street
drug use, and lifetime number of sexual partners.
Adjusted for all characteristics in the previous 2 footnotes in addition to hepatitis C virus, HIV, and herpes simplex virus 2 status.
Category includes ages 20 to 29 y for the adjusted ORs limited to persons aged 20 y.
Includes Mexican Americans and other Hispanic persons.
Only men aged 17 y are presented in the univariate analyses.
** Antibody to hepatitis C virus confirmed by recombinant immunoblot assay.
United States had a particularly high prevalence of exposure to HBV, especially if they were not white, black, or
Hispanic (31.3%). The prevalence of exposure to HBV
increased dramatically with age and was higher in persons with low family income and low educational attainment. Consistent with known methods of HBV transmission, persons who reported intravenous drug use or
numerous sexual partners had a particularly high prevalence of exposure to HBV. Persons with serologic evidence of exposure to other hematogenous or sexually
transmitted viruses (HIV, hepatitis C virus [HCV], or
herpes simplex virus 2) had a very high prevalence of
exposure to HBV. Blood transfusion, even before 1991,
was associated with only a slightly increased prevalence
of exposure to HBV.
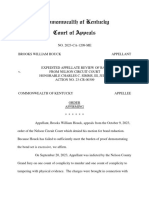
Figures 1 and 2 show that up to a 50-fold change in
the prevalence of exposure to HBV was observed as age,
race, and ethnicity varied or as age and country of birth
varied. Although exposure to HBV is very uncommon
(1%) in persons aged 6 to 19 years, regardless of race or
ethnicity or country of birth, the rate is more than 9%
among black persons aged 50 years or older, more than
30% among persons of other racial or ethnic groups who
are aged 50 years or older, and more than 43% in persons
of other race or ethnicity born outside the United States
who are aged 50 years or older.
www.annals.org
Non-Hispanic black persons and persons of other race
or ethnicity, who constituted only 11.4% and 5.3% of the
U.S. population, accounted for 26% and 21% of all persons exposed to HBV and 31% and 39% of all persons
with chronic HBV infection, respectively. Persons born
outside the United States or Mexico, who made up only
9.5% of the U.S. population, constituted 34.4% of all
persons exposed to HBV and 46.4% of all persons with
chronic HBV infection. Categorized into mutually exclusive categories, the following groups accounted for the majority (56%) of HBV-exposed persons in the United States:
non-Hispanic black persons born in the United States
(21%); persons of white, black, or Hispanic race or ethnicity born outside the United States (17%); and persons of
other race or ethnicity born outside the United States
(18%).
Among children aged 2 years (n 685), 68.6% (CI,
64.1% to 73.2%) had positive serum anti-HBs titers,
whereas among children aged 3, 4, and 5 years, the respective rates were 58.7% (CI, 54.2% to 63.2%), 56.6% (CI,
51.9% to 61.3%), and 52.1% (CI, 53.9% to 58.6%). Little difference was observed in the prevalence of anti-HBs
among children aged 2 years by sex, race or ethnicity, and
family income (data not shown).
Among persons aged 6 years or older, the prevalence
of positive anti-HBs in the absence of anti-HBc (a pos1 March 2011 Annals of Internal Medicine Volume 154 Number 5 325
Hepatitis B Virus in the United States: Infection, Exposure and Immunity Rates
Figure 1. Prevalence of anti-HBc in the U.S. population, by
age and race or ethnicity.
60
Anti-HBcPositive Persons, %
50
40
30
20
10
0
619
2029
3039
4049
5059
6069
70
Age Group, y
Hispanic
Other
Black
White
anti-HBc antibody to hepatitis B core antigen.
itive anti-HBs and negative anti-HBc), suggestive of
persistent presence of protective antibodies after vaccination, was 22.6% (Table 3). This prevalence was much
higher in persons aged 13 to 17 years (62.4%) and decreased rapidly in older age groups to 3.7% in persons
aged 70 years or older. Men were less likely than women
to test positive for anti-HBs and negative for anti-HBc.
Persons at particularly high risk for HBV infection, such
as persons reporting several sexual partners or street
drug use and persons exposed to HIV, HCV, or herpes
simplex virus 2, had a lower prevalence of a positive
anti-HBs and negative anti-HBc titer than persons without these risk factors.
DISCUSSION
The prevalence of chronic HBV infection in the
United States from 1999 to 2008 was 0.27% (CI, 0.20%
to 0.34%) among persons aged 6 years or older, corresponding to 704 000 persons. This estimate is slightly
lower than previous national estimates from 1976 to 1980
(0.33% [CI, 0.21% to 0.51%]) or 1988 to 1994 (0.42%
[CI, 0.32% to 0.44%]) (1). The prevalence of exposure to
HBV (past or chronic infection) from 1999 to 2008 was
4.6% (CI, 4.1% to 5.0]), corresponding to 11 993 999
persons. This estimate is also lower than previous national
estimates from 1976 to 1980 (5.5% [CI, 4.8 to 6.2]) or
1988 to 1994 (5.1% [CI, 4.4 to 5.8]).
Guidelines for universal childhood vaccination were
published in 1991, federal programs for routine vaccination of infants began in late 1992, and vaccination of adolescents who were not vaccinated as infants was included
326 1 March 2011 Annals of Internal Medicine Volume 154 Number 5
in the Vaccines for Children program in 1995. The Advisory Committee on Immunization Practices additionally
recommends routine screening of all pregnant women,
postexposure immunoprophylaxis of infants born to
HBsAg-positive women, and vaccination of adults at increased risk for infection (2, 18). The modest decline in
HBV infection and exposure that is reported herein may be
related to these immunization efforts. Even if universal
childhood vaccination had been achieved since 1992, more
dramatic reductions in infection and exposure rates would
not have been expected by the study period (1999 to 2008)
because children vaccinated since 1992 have not yet
reached adulthood when most exposure to HBV occurs in
the United States.
Most cases of HBV infection or exposure in the
United States occur among black persons or persons of
other race or ethnicity (primarily Asian) and persons born
outside the United States. Therefore, race, ethnicity, and
country of birth are the most important epidemiologic correlates of HBV infection in the United States.
Exposure to HBV in the United States is very low
among persons aged 18 years or younger (0.5%) and increases with age thereafter. This is true even among persons
of other race or ethnicity (mostly Asian), suggesting that
little exposure to HBV occurred in the United States in the
past 20 years as a result of vertical or perinatal transmission, even among Asian persons. Rather, most exposure to
HBV in the United States occurs in adulthood as a result
of sexual intercourse or intravenous drug use.
Figure 2. Prevalence of anti-HBc, by age and birthplace.
70
60
Anti-HBcPositive Persons, %
Original Research
50
40
30
20
10
0
619
2029
3039
4049
5059
6069
70
Age Group, y
Mexico
Elsewhere
(other)
Elsewhere
(white, black, Hispanic)
United
States
anti-HBc antibody to hepatitis B core antigen.
www.annals.org
Hepatitis B Virus in the United States: Infection, Exposure and Immunity Rates
Exposure to HBV (past or chronic infection) in the
U.S. population is 17 times more common than chronic
infection, consistent with the fact that most persons who
are exposed to HBV in adulthood are able to clear the
virus without persistence of HBsAg in serum. However,
exposure to HBV is an important epidemiologic parameter, even in the absence of serum HBsAg, because such
persons, who may retain the HBV genome indefinitely in
previously infected liver cells, are susceptible to HBV reactivation (especially in the setting of immunosuppression)
and may have an increased risk for cirrhosis or hepatocellular carcinoma (19 22). Even if the excess risk for adverse
outcomes associated with previous exposure is low, this
may still have a substantial effect on public health because
of the very large number of persons (about 11 993 000) in
the United States who have been exposed to HBV.
The reported prevalence of serum anti-HBs levels
greater than 10 IU/L among children aged 2 years in the
United States that is reported (68.6%) is substantially
lower than the proportion of children aged 19 to 35
months who were previously reported to have received at
least 3 doses of HBV vaccine in the United States from
2004 to 2009 (92.4% to 93.5%) (3, 4). This difference
might be due to children not developing adequate levels of
anti-HBs (10 IU/L) after vaccination or due to a decline
in anti-HBs levels to 10 IU/L or less, which may occur
even in the short period between completion of the infant
HBV vaccination series (usually between age 12 and 18
months) and measurement of anti-HBs in NHANES participants aged 2 years. The prevalence of serum anti-HBs
in children aged 3, 4, and 5 years further decreased to
58.7%, 56.6%, and 52.1%, respectively, suggesting substantial loss of serum anti-HBs within the first 3 to 4 years
after vaccination. Similarly, the prevalence of anti-HBs levels greater than 10 IU/L among adolescents aged 13 to 17
years reported here (62.4%) is much lower than the proportion of adolescents aged 13 to 17 years reported to have
received at least 3 doses of HBV vaccination in the United
States from 2007 to 2009 (87.6% to 89.9%) (23, 24).
These findings will be useful as knowledge continues to
accumulate about whether persons who lose anti-HBs after
vaccination continue to have effective protection against
HBV infection and persistence or whether they require
booster vaccination (6, 12, 25). If the latter is determined to
be the case, then the data presented here can be used to estimate the proportion of adolescents and young adults who
may require booster vaccination (which is currently not
recommended).
Current immunization recommendations also include
vaccination of adults at increased risk for infection, such
as patients with HIV (26) or HCV infection (27) and
persons who report a history of several sex partners, treatment for sexually transmitted diseases, and injection-drug
use (2, 18, 28). This is important to limit transmission of
HBV between adults until the current cohorts of vaccinated children reach adulthood. However, the current
www.annals.org
Original Research
findings suggest that certain high-risk groups are actually
less likely to have serum anti-HBs in the absence of antiHBc, such as persons reporting several sexual partners or
intravenous drug use and persons exposed to HIV, HCV,
or herpes simplex virus 2. Other studies suggest that more
than one half of the reported cases of acute hepatitis B in
the United States occurred in persons who had previously
received care in sexually transmitted disease clinics or correctional facilities (29). Taken together with past studies,
the current results highlight the need for better mechanisms to both reach and offer vaccination to these high-risk
groups.
This study has limitations. NHANES neither oversampled nor specifically identified Asian races or ethnicities
that have high prevalence of HBV. Instead, other race or
ethnicity denoted all participants who were not white,
black, Hispanic, or Mexican. This precluded estimation of
HBV prevalence among specific Asian races or ethnicities
in the United States. The oversampling of black and Hispanic persons and lack of oversampling of Asian persons
should not necessarily bias estimates of the prevalence of
HBV exposure and infection in the United States reported
here, because weights are provided and were used to account for the deliberate oversampling of certain racial or
demographic groups. However, it is possible that certain
high-risk groups, such as recently arrived or unauthorized
Asian immigrants, were not accurately accounted for by
the NHANES sampling and weighting schemes, leading to
underestimation in the national estimates of HBV exposure and infection. The sampling frame of NHANES did
not include incarcerated or homeless persons. Approximately 2% of incarcerated inmates (about 34 000 persons)
were chronically infected with HBV in 1997 (30). If these
persons were added to the 704 000 persons that were estimated to have HBV, the total number of persons with
chronic infection would increase to 738 000, or 0.28%
(instead of 0.27%). Among homeless veterans hospitalized
at a Veterans Administration domiciliary from 1995 to
2000 who were also be tested for HBV infection, 1.17%
had a positive result (31). The exclusion of homeless and
incarcerated persons from NHANES means that the true
national HBV prevalence was slightly underestimated.
From Veterans Affairs Puget Sound Health Care System and University
of Washington, Seattle, Washington.
Disclaimer: Dr. Ioannou had full access to all of the data in the study
and takes responsibility for the integrity and the accuracy of the data
analysis. Dr. Ioannou was responsible for study concept and design,
acquisition of data, analysis and interpretation of the data, and drafting
of the manuscript.
Grant Support: By the Veterans Affairs Research Enhancement Award
Program.
Potential Conflicts of Interest: Disclosures can be viewed at www.acponline
.org/authors/icmje/ConflictOfInterestForms.do?msNumM10-1301.
1 March 2011 Annals of Internal Medicine Volume 154 Number 5 327
Original Research
Hepatitis B Virus in the United States: Infection, Exposure and Immunity Rates
Reproducible Research Statement: Study protocol, statistical code, and
data set: Not available.
Corresponding Author: George N. Ioannou, BMBCh, MS, Veterans
Affairs Puget Sound Health Care System, Gastroenterology, S-111Gastro, 1660 South Columbian Way, Seattle, WA 98108; e-mail,
georgei@medicine.washington.edu.
Author contributions are available at www.annals.org.
References
1. McQuillan GM, Coleman PJ, Kruszon-Moran D, Moyer LA, Lambert SB,
Margolis HS. Prevalence of hepatitis B virus infection in the United States: the
National Health and Nutrition Examination Surveys, 1976 through 1994. Am J
Public Health. 1999;89:14-8. [PMID: 9987458]
2. Hepatitis B virus: a comprehensive strategy for eliminating transmission in the
United States through universal childhood vaccination. Recommendations of the
Immunization Practices Advisory Committee (ACIP). MMWR Recomm Rep.
1991;40:1-25. [PMID: 1835756]
3. Centers for Disease Control and Prevention (CDC). National, state, and local
area vaccination coverage among children aged 19-35 months-United States,
2009. MMWR Morb Mortal Wkly Rep. 2010;59:1171-7. [PMID: 20847720]
4. Centers for Disease Control and Prevention (CDC). National, state, and local
area vaccination coverage among children aged 19-35 monthsUnited States,
2008. MMWR Morb Mortal Wkly Rep. 2009;58:921-6. [PMID: 19713881]
5. Gabbuti A, Romano` L, Blanc P, Meacci F, Amendola A, Mele A, et al.
Long-term immunogenicity of hepatitis B vaccination in a cohort of Italian
healthy adolescents. Vaccine. 2007;25:3129-32. [PMID: 17291637]
6. Hall AJ. Boosters for hepatitis B vaccination? Need for an evidence-based
policy [Editorial]. Hepatology. 2010;51:1485-6. [PMID: 20432250]
7. McMahon BJ, Bruden DL, Petersen KM, Bulkow LR, Parkinson AJ,
Nainan O, et al. Antibody levels and protection after hepatitis B vaccination:
results of a 15-year follow-up. Ann Intern Med. 2005;142:333-41. [PMID:
15738452]
8. Van Damme P, von Sonnenburg F, Hatz C, Hoet B, Lefevre I, Leyssen M.
Long-term immunogenicity of preservative-free hepatitis B vaccine formulations
in adults. J Med Virol. 2009;81:1710-5. [PMID: 19697416]
9. Lin YC, Chang MH, Ni YH, Hsu HY, Chen DS. Long-term immunogenicity and efficacy of universal hepatitis B virus vaccination in Taiwan. J Infect Dis.
2003;187:134-8. [PMID: 12508157]
10. Zanetti AR, Mariano A, Romano` L, DAmelio R, Chironna M, Coppola
RC, et al; Study Group. Long-term immunogenicity of hepatitis B vaccination
and policy for booster: an Italian multicentre study. Lancet. 2005;366:1379-84.
[PMID: 16226616]
11. Lu CY, Ni YH, Chiang BL, Chen PJ, Chang MH, Chang LY, et al.
Humoral and cellular immune responses to a hepatitis B vaccine booster 15-18
years after neonatal immunization. J Infect Dis. 2008;197:1419-26. [PMID:
18444799]
12. Van Damme P, Van Herck K. A review of the long-term protection after
hepatitis A and B vaccination. Travel Med Infect Dis. 2007;5:79-84. [PMID:
17298912]
13. Laboratory Procedure Manual, Antibody to Hepatitis B Surface Antigen
in Serum, NHANES. Accessed at www.cdc.gov/nchs/data/nhanes/nhanes
_05_06/hepb_s_d_met_hep_b_surface_antibody.pdf on 17 May 2010.
14. Bauer T, Jilg W. Hepatitis B surface antigen-specific T and B cell memory in
328 1 March 2011 Annals of Internal Medicine Volume 154 Number 5
individuals who had lost protective antibodies after hepatitis B vaccination. Vaccine. 2006;24:572-7. [PMID: 16171909]
15. Analytic and reporting guidelines. The National Health and Nutrition Examination Survey (NHANES). Hyattsville, MD: National Center for Health
Statistics. Accessed at www.cdc.gov/nchs/data/nhanes/nhanes_03_04/nhanes
_analytic_guidelines_dec_2005.pdf on 21 April 2010.
16. Korn EL, Graubard BI. Analysis of Health Surveys. New York: Wiley; 1999:
75-76.
17. U.S. Census Bureau. United States Census 2000. Accessed at www.census
.gov/main/www/cen2000.html on 19 May 2010.
18. Centers for Disease Control and Prevention (CDC). Update: recommendations to prevent hepatitis B virus transmissionUnited States. MMWR Morb
Mortal Wkly Rep. 1995;44:574-5. [PMID: 7616955]
19. Cacciola I, Pollicino T, Squadrito G, Cerenzia G, Orlando ME, Raimondo
G. Occult hepatitis B virus infection in patients with chronic hepatitis C liver
disease. N Engl J Med. 1999;341:22-6. [PMID: 10387938]
20. Pollicino T, Squadrito G, Cerenzia G, Cacciola I, Raffa G, Craxi A, et al.
Hepatitis B virus maintains its pro-oncogenic properties in the case of occult
HBV infection. Gastroenterology. 2004;126:102-10. [PMID: 14699492]
21. Ioannou GN, Splan MF, Weiss NS, McDonald GB, Beretta L, Lee SP.
Incidence and predictors of hepatocellular carcinoma in patients with cirrhosis.
Clin Gastroenterol Hepatol. 2007;5:938-45, 945.e1-4. [PMID: 17509946]
22. Urbani S, Fagnoni F, Missale G, Franchini M. The role of anti-core antibody response in the detection of occult hepatitis B virus infection. Clin Chem
Lab Med. 2010;48:23-9. [PMID: 19919328]
23. Centers for Disease Control and Prevention (CDC). National, state, and
local area vaccination coverage among adolescents aged 13-17 years-United
States, 2009. MMWR Morb Mortal Wkly Rep. 2010;59:1018-23. [PMID:
20724968]
24. Centers for Disease Control and Prevention (CDC). National, state, and
local area vaccination coverage among adolescents aged 13-17 yearsUnited
States, 2008. MMWR Morb Mortal Wkly Rep. 2009;58:997-1001. [PMID:
19763075]
25. Kao JH, Chen DS. Hepatitis B vaccination: to boost or not to boost? Lancet.
2005;366:1337-8. [PMID: 16226597]
26. Kaplan JE, Benson C, Holmes KH, Brooks JT, Pau A, Masur H; Centers
for Disease Control and Prevention (CDC). Guidelines for prevention and
treatment of opportunistic infections in HIV-infected adults and adolescents:
recommendations from CDC, the National Institutes of Health, and the HIV
Medicine Association of the Infectious Diseases Society of America. MMWR
Recomm Rep. 2009;58:1-207; quiz CE1-4. [PMID: 19357635]
27. Ghany MG, Strader DB, Thomas DL, Seeff LB; American Association for
the Study of Liver Diseases. Diagnosis, management, and treatment of hepatitis
C: an update. Hepatology. 2009;49:1335-74. [PMID: 19330875]
28. Alter MJ. Epidemiology and prevention of hepatitis B. Semin Liver Dis.
2003;23:39-46. [PMID: 12616449]
29. Goldstein ST, Alter MJ, Williams IT, Moyer LA, Judson FN, Mottram K,
et al. Incidence and risk factors for acute hepatitis B in the United States, 19821998: implications for vaccination programs. J Infect Dis. 2002;185:713-9.
[PMID: 11920288]
30. Weinbaum C, Lyerla R, Margolis HS; Centers for Disease Control and
Prevention. Prevention and control of infections with hepatitis viruses in correctional settings. Centers for Disease Control and Prevention. MMWR Recomm
Rep. 2003;52:1-36. [PMID: 12562146]
31. Cheung RC, Hanson AK, Maganti K, Keeffe EB, Matsui SM. Viral hepatitis and other infectious diseases in a homeless population. J Clin Gastroenterol.
2002;34:476-80. [PMID: 11907367]
www.annals.org
Annals of Internal Medicine
Author Contributions: Conception and design: G.N. Ioannou.
Analysis and interpretation of the data: G.N. Ioannou.
Drafting of the article: G.N. Ioannou.
Critical revision of the article for important intellectual content: G.N.
Ioannou.
Final approval of the article: G.N. Ioannou.
Statistical expertise: G.N. Ioannou.
Obtaining of funding: G.N. Ioannou.
Collection and assembly of data: G.N. Ioannou.
APPENDIX: COMPARISON OF HBV INFECTION AND
EXPOSURE PREVALENCE FROM NHANES III (1988
1994) AND NHANES, 1999 TO 2008
TO
The prevalence of exposure to HBV (anti-HBc) in
NHANES III (1988 to 1994) was reported by McQuillan and
colleagues (1) as 4.9% among persons aged 6 to 74 years (the
value reported in their abstract) and 5.1% among persons 6 years
or older, with no upper age limit (the value reported in Table 2
of their article). The prevalence of chronic HBV infection (HBsAg) was reported as 0.42% among persons aged 6 to 74 years,
whereas the prevalence among all persons aged 6 years or older
was not reported. These estimates were age-adjusted by the direct
method to the 1980 census U.S. population.
I calculated the prevalence of HBV exposure and infection
by using NHANES III (1988 to 1994) data for all persons 6
years or older with and without standardizing (age and sex) to the
2000 U.S. population census, so that results would be similar to
those that I presented for NHANES 1999 to 2008. These results
are shown in the Appendix Table. The differences between
NHANES III and NHANES 1999 to 2008 are that standardized
prevalences of anti-HBc and HBsAg were both statistically significant (P 0.001).
Because the prevalence of anti-HBc and HBsAg from
NHANES III are published elsewhere (albeit standardized to the
1980 census U.S. population), an analysis of the NHANES III
data was not included here because of space constraints.
Appendix Table. Hepatitis B Virus Infection and Exposure Prevalence From NHANES III (1988 to 1994) and NHANES 1999 to 2008
NHANES Period
19881994
19992008
Participants, n
21 260
37 259
Data Not Standardized
Data Standardized to 2000 U.S.
Census Population
HBsAg
(95% CI), %
Anti-HBc
(95% CI), %
HBsAg
(95% CI), %
Anti-HBc
(95% CI), %
0.38 (0.280.48)
0.27 (0.200.34)
5.3 (4.76.0)
4.6 (4.15.0)
0.38 (0.280.42)
0.26 (0.190.34)
5.5 (4.85.2)
4.4 (4.04.9)
anti-HBc antibody against hepatitis B core antigen; HBsAg hepatitis B surface antigen; NHANES National Health and Nutrition Examination Survey.
W-98 1 March 2011 Annals of Internal Medicine Volume 154 Number 5
www.annals.org
Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Pages From Nathaniel Samuel Murrell - Afro-Caribbean ReligionsDokument73 SeitenPages From Nathaniel Samuel Murrell - Afro-Caribbean ReligionsMilesErohs100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Ten Personality Disorders - Neel Burton MDDokument11 SeitenTen Personality Disorders - Neel Burton MDcgarciNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- CounterfeitingDokument21 SeitenCounterfeitingnujahm1639Noch keine Bewertungen
- 2023 Commercial and Taxation LawsDokument7 Seiten2023 Commercial and Taxation LawsJude OnrubiaNoch keine Bewertungen
- The Digital Future FinanceDokument17 SeitenThe Digital Future FinanceMid VillepinteNoch keine Bewertungen
- Plant Kingdom EssentHomoeopDokument40 SeitenPlant Kingdom EssentHomoeopcgarciNoch keine Bewertungen
- Endocrino and HomeopathyDokument24 SeitenEndocrino and HomeopathycgarciNoch keine Bewertungen
- Matridonal Remedies LGraystonDokument9 SeitenMatridonal Remedies LGraystonaruen79100% (1)
- List of Mumbai SchoolsDokument10 SeitenList of Mumbai Schoolsapi-3714390100% (4)
- Relationship of Remedies DR Rgibson Miller PDFDokument9 SeitenRelationship of Remedies DR Rgibson Miller PDFcgarci100% (3)
- Arsenicum Alb - Holistic LookDokument3 SeitenArsenicum Alb - Holistic LookcgarciNoch keine Bewertungen
- Atlas Rutier Romania by Constantin FurtunaDokument4 SeitenAtlas Rutier Romania by Constantin FurtunaAntal DanutzNoch keine Bewertungen
- Asafoetida AsafDokument49 SeitenAsafoetida AsafcgarciNoch keine Bewertungen
- ProfJutte Lowpotencies PDFDokument6 SeitenProfJutte Lowpotencies PDFcgarciNoch keine Bewertungen
- Natrum Mur FarringtonDokument16 SeitenNatrum Mur FarringtoncgarciNoch keine Bewertungen
- Immune SuppressionDokument1 SeiteImmune SuppressioncgarciNoch keine Bewertungen
- Cerebral ParesisCase Berridge.Dokument3 SeitenCerebral ParesisCase Berridge.cgarciNoch keine Bewertungen
- Gwillim, Linda & Biggs, Kathy - Placenta HumanumDokument90 SeitenGwillim, Linda & Biggs, Kathy - Placenta HumanumLeonard MichlinNoch keine Bewertungen
- Marketing PlanDokument52 SeitenMarketing PlanRaissa MaeNoch keine Bewertungen
- Affidavit of Probable Cause: ArresteeDokument3 SeitenAffidavit of Probable Cause: ArresteeMcKenzie StaufferNoch keine Bewertungen
- Art Region 3Dokument49 SeitenArt Region 3JB LicongNoch keine Bewertungen
- Family Chapter Revision GuideDokument9 SeitenFamily Chapter Revision GuidePuss BootNoch keine Bewertungen
- FEMADokument51 SeitenFEMAChinmay Shirsat50% (2)
- Metaswitch Datasheet Perimeta SBC OverviewDokument2 SeitenMetaswitch Datasheet Perimeta SBC OverviewblitoNoch keine Bewertungen
- Problem 5 Acctg7Dokument5 SeitenProblem 5 Acctg7Nyster Ann RebenitoNoch keine Bewertungen
- Module 2Dokument30 SeitenModule 2RarajNoch keine Bewertungen
- BTL VĨ Mô Chuyên SâuDokument3 SeitenBTL VĨ Mô Chuyên SâuHuyền LinhNoch keine Bewertungen
- Omega Temp and Humidity Manual MQS4098Dokument2 SeitenOmega Temp and Humidity Manual MQS4098BSC-566731Noch keine Bewertungen
- School Calendar Version 2Dokument1 SeiteSchool Calendar Version 2scituatemarinerNoch keine Bewertungen
- Arab Americans and Political ActivismDokument4 SeitenArab Americans and Political ActivismRaouia ZouariNoch keine Bewertungen
- CCES Guide 2018Dokument117 SeitenCCES Guide 2018Jonathan RobinsonNoch keine Bewertungen
- Accessing Resources For Growth From External SourcesDokument14 SeitenAccessing Resources For Growth From External SourcesHamza AdilNoch keine Bewertungen
- Summer Internship ProjectDokument52 SeitenSummer Internship ProjectJaskaran SinghNoch keine Bewertungen
- Invoice: Issue Date Due DateDokument2 SeitenInvoice: Issue Date Due DateCheikh Ahmed Tidiane GUEYENoch keine Bewertungen
- Trading in BinanceDokument11 SeitenTrading in BinancededithegamingNoch keine Bewertungen
- Glo 20is 2017 PDFDokument317 SeitenGlo 20is 2017 PDFKristine LlamasNoch keine Bewertungen
- Taras Tymchuk CVDokument1 SeiteTaras Tymchuk CVТарас ТимчукNoch keine Bewertungen
- Resting in The RiverDokument4 SeitenResting in The RiverNguyễn Văn TưởngNoch keine Bewertungen
- Court of Appeals Order AffirmingDokument16 SeitenCourt of Appeals Order AffirmingLisa AutryNoch keine Bewertungen
- Development of Science and Technology in The PhilippinesDokument12 SeitenDevelopment of Science and Technology in The PhilippinesJyra Shael L. EscanerNoch keine Bewertungen
- Assistant Sub Inspector (BS-09) Anti Corruption Establishment Punjab 16 C 2020 PDFDokument3 SeitenAssistant Sub Inspector (BS-09) Anti Corruption Establishment Punjab 16 C 2020 PDFAgha Khan DurraniNoch keine Bewertungen
- G.R. No. 133154. December 9, 2005. JOWEL SALES, Petitioner, vs. CYRIL A. SABINO, RespondentDokument6 SeitenG.R. No. 133154. December 9, 2005. JOWEL SALES, Petitioner, vs. CYRIL A. SABINO, RespondentJoshua Erik MadriaNoch keine Bewertungen