Das könnte Ihnen auch gefallen
- Amazon PrimeDokument27 SeitenAmazon PrimeMohamedNoch keine Bewertungen
- Baby Romper Pattern and Sewing Tutorial 2014Dokument18 SeitenBaby Romper Pattern and Sewing Tutorial 2014Carolina Ribeiro100% (1)
- Em Swedenborg THE WORD EXPLAINED Volume IX INDICES Academy of The New Church Bryn Athyn PA 1951Dokument236 SeitenEm Swedenborg THE WORD EXPLAINED Volume IX INDICES Academy of The New Church Bryn Athyn PA 1951francis batt100% (2)
- Mircea Eliade and Ernst Jünger On Human Sacrifice, 1937-1945Dokument31 SeitenMircea Eliade and Ernst Jünger On Human Sacrifice, 1937-1945Direktor Kile100% (1)
- Epidemiology in A Nutshell NCI BenchmarksDokument8 SeitenEpidemiology in A Nutshell NCI BenchmarksThe Nutrition CoalitionNoch keine Bewertungen
- Oblicon NotesDokument14 SeitenOblicon NotesCee Silo Aban100% (1)
- Modal VerbsDokument2 SeitenModal VerbsDICX7770% (1)
- Master of Science in Health Development: Critical Appraisal of Prognostic StudyDokument14 SeitenMaster of Science in Health Development: Critical Appraisal of Prognostic StudyHappy Ary SatyaniNoch keine Bewertungen
- Letter To The EditorsDokument2 SeitenLetter To The EditorsLodika HandayaniNoch keine Bewertungen
- 10 KotepuiDokument5 Seiten10 KotepuiAlfeus GradyNoch keine Bewertungen
- Passive Smoking and Cervical Cancer Risk: A Meta-Analysis Based On 3,230 Cases and 2,982 ControlsDokument7 SeitenPassive Smoking and Cervical Cancer Risk: A Meta-Analysis Based On 3,230 Cases and 2,982 ControlsarnalordNoch keine Bewertungen
- 2-Jankovic (4-12)Dokument9 Seiten2-Jankovic (4-12)Okki Masitah Syahfitri NasutionNoch keine Bewertungen
- PIIS0022202X1536098XDokument9 SeitenPIIS0022202X1536098XcutfarahputheNoch keine Bewertungen
- 429 FullDokument9 Seiten429 Fullgrum jawNoch keine Bewertungen
- IJSRMDokument11 SeitenIJSRMjaya kumarNoch keine Bewertungen
- Precisión de La Información Del Cáncer de Mama en Internet: Análisis de ContenidoDokument5 SeitenPrecisión de La Información Del Cáncer de Mama en Internet: Análisis de ContenidoDaniel Hidalgo HernandezNoch keine Bewertungen
- Just The Facts Epidemiology and EtologyDokument18 SeitenJust The Facts Epidemiology and EtologyOtto LancelleNoch keine Bewertungen
- Modified Physologic IndexDokument8 SeitenModified Physologic Indexbin linNoch keine Bewertungen
- Studying The Prevalence of Risk Factors For Some Major Noncommunicable Diseases Among The Women PopulationDokument7 SeitenStudying The Prevalence of Risk Factors For Some Major Noncommunicable Diseases Among The Women PopulationCentral Asian StudiesNoch keine Bewertungen
- Original Article3 PDFDokument6 SeitenOriginal Article3 PDFTriponiaNoch keine Bewertungen
- Issn: 0976-3325Dokument3 SeitenIssn: 0976-3325karina chaswinNoch keine Bewertungen
- Djimeu Published Replication PlanDokument17 SeitenDjimeu Published Replication PlanVishalvishaldograNoch keine Bewertungen
- Daño InglesDokument9 SeitenDaño InglesbrukillmannNoch keine Bewertungen
- Clinical Epidemiology and Global Health: Pragati Sharma, Sanjay M. PattanshettyDokument5 SeitenClinical Epidemiology and Global Health: Pragati Sharma, Sanjay M. PattanshettyIzzati Filza RahmadeaNoch keine Bewertungen
- 1953 PDFDokument4 Seiten1953 PDFHesti hasanNoch keine Bewertungen
- The New England Journal of MedicineDokument12 SeitenThe New England Journal of MedicineElyzabeth BonnesNoch keine Bewertungen
- Eli SpotDokument20 SeitenEli SpotAdel HamadaNoch keine Bewertungen
- LSHTM Study Designs NOTES LSTHMDokument39 SeitenLSHTM Study Designs NOTES LSTHMKELVIN MAYOMBONoch keine Bewertungen
- VM 2073 Review of Use of Evidence (Epidemiology) Years 1 And2Dokument61 SeitenVM 2073 Review of Use of Evidence (Epidemiology) Years 1 And2KerolusMouradNoch keine Bewertungen
- Oup Accepted Manuscript 2018Dokument7 SeitenOup Accepted Manuscript 2018FaidurrahmanNoch keine Bewertungen
- Downloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Dokument28 SeitenDownloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Indah Putri permatasariNoch keine Bewertungen
- Journal Pre-Proof: Annals of OncologyDokument6 SeitenJournal Pre-Proof: Annals of OncologySyia Rasyia D'feeitaNoch keine Bewertungen
- The Prevalence of Polycystic Ovary Syndrome in A Community Sample Assessed Under Contrasting Diagnostic CriteriaDokument8 SeitenThe Prevalence of Polycystic Ovary Syndrome in A Community Sample Assessed Under Contrasting Diagnostic CriteriaKe XuNoch keine Bewertungen
- Expo Cervantes 2Dokument31 SeitenExpo Cervantes 2Alfredo Nano VieyraNoch keine Bewertungen
- Lepra Pada AnakDokument5 SeitenLepra Pada AnakAdrian AldrinNoch keine Bewertungen
- 76 157 1 SM PDFDokument15 Seiten76 157 1 SM PDFPin Han NaNoch keine Bewertungen
- Kou Kou 2023 Severity and Risk Factors of Interval Breast Cancer in QueenslandDokument21 SeitenKou Kou 2023 Severity and Risk Factors of Interval Breast Cancer in Queenslandalison.koukouNoch keine Bewertungen
- Nwalozie RMdoiideDokument11 SeitenNwalozie RMdoiideijmb333Noch keine Bewertungen
- Celecoxib For The Prevention of Colorectal Adenomatous PolypsDokument11 SeitenCelecoxib For The Prevention of Colorectal Adenomatous PolypsJae Yong LeeNoch keine Bewertungen
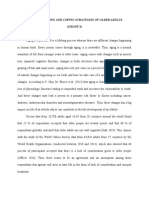
- Effects of Aging and Coping Strategies of Older Adults (GROUP 3)Dokument16 SeitenEffects of Aging and Coping Strategies of Older Adults (GROUP 3)Michael AmandyNoch keine Bewertungen
- Rockson Ohene Asante 2235026 - Epidemiology Assignment by Pratap Kumar Jena SirDokument11 SeitenRockson Ohene Asante 2235026 - Epidemiology Assignment by Pratap Kumar Jena SirRockson Ohene AsanteNoch keine Bewertungen
- Copia de Final 2019-2020 No Answers PDFDokument20 SeitenCopia de Final 2019-2020 No Answers PDFadkfnlsºNoch keine Bewertungen
- EpidemiologyDokument36 SeitenEpidemiologyhendra2darmawan50% (2)
- Faktor-Faktor Yang Mempengaruhi Kualitas Hidup Penderita Kanker Payudara Di Kota PadangDokument6 SeitenFaktor-Faktor Yang Mempengaruhi Kualitas Hidup Penderita Kanker Payudara Di Kota Padangbenny wibowoNoch keine Bewertungen
- EndometriosisDokument13 SeitenEndometriosisDian NovitaNoch keine Bewertungen
- Knowledge Regarding Cervical Cancer Among Married Women in Rural Telangana: A Cross Sectional StudyDokument5 SeitenKnowledge Regarding Cervical Cancer Among Married Women in Rural Telangana: A Cross Sectional StudySrideviRaviNoch keine Bewertungen
- Prevalence and Risk Factors of Abortion Among Women in Ksa: A Cross - Sectional StudyDokument20 SeitenPrevalence and Risk Factors of Abortion Among Women in Ksa: A Cross - Sectional StudyIJAR JOURNALNoch keine Bewertungen
- Pulmonary Nontuberculous Mycobacterial Disease Prevalence and Clinical FeaturesDokument6 SeitenPulmonary Nontuberculous Mycobacterial Disease Prevalence and Clinical FeaturesRiski DohartuaNoch keine Bewertungen
- Jid 2009113 ADokument9 SeitenJid 2009113 AAMELIA.SYAHUTAMINoch keine Bewertungen
- Epidemiology of Leprosy. in Book - Textbook of Clinical Leprosy Chapter 1.1 ITL - 1 - 1FINALDokument29 SeitenEpidemiology of Leprosy. in Book - Textbook of Clinical Leprosy Chapter 1.1 ITL - 1 - 1FINALNaeNoch keine Bewertungen
- BayyapareddyDokument8 SeitenBayyapareddyeditorijmrhsNoch keine Bewertungen
- Risk Factors For Otitis Media in Rural, Preschool South Indian ChildrenDokument20 SeitenRisk Factors For Otitis Media in Rural, Preschool South Indian ChildrengoolnuulNoch keine Bewertungen
- Detection of Breast Cancer in Mousl CityDokument16 SeitenDetection of Breast Cancer in Mousl CityHama karimNoch keine Bewertungen
- Testis PDFDokument8 SeitenTestis PDFVlatka MartinovichNoch keine Bewertungen
- Review ArticleDokument14 SeitenReview ArticlePanji Agung KhrisnaNoch keine Bewertungen
- Antidepressant Medication Use and Breast Cancer RiskDokument6 SeitenAntidepressant Medication Use and Breast Cancer RiskinloesNoch keine Bewertungen
- Research: ArticleDokument4 SeitenResearch: ArticleMuthu KumarNoch keine Bewertungen
- Simanjuntak, 2023Dokument8 SeitenSimanjuntak, 2023Ivo TrisnaNoch keine Bewertungen
- Ovario Poliquitico ArticuloDokument6 SeitenOvario Poliquitico ArticuloDaniela CristanchoNoch keine Bewertungen
- Oral Epidemiology: Epidemiology. Dr. Mohamed Al-MontaserDokument58 SeitenOral Epidemiology: Epidemiology. Dr. Mohamed Al-Montaserغلاها عبدوNoch keine Bewertungen
- Manuel Posada InglsDokument12 SeitenManuel Posada InglsMarieta Díez-JuanNoch keine Bewertungen
- Jurnal 2Dokument16 SeitenJurnal 2Edwin Pasha Jr.Noch keine Bewertungen
- Title Group B Streptococcal Infection in Non-Pregnant AdultsDokument17 SeitenTitle Group B Streptococcal Infection in Non-Pregnant AdultsHam FGNoch keine Bewertungen
- A Randomized Trial of Multivitamin Supplements and HIV Disease Progression and MortalityDokument10 SeitenA Randomized Trial of Multivitamin Supplements and HIV Disease Progression and MortalityNugrohoNoch keine Bewertungen
- Cancer Entangled: Anticipation, Acceleration, and the Danish StateVon EverandCancer Entangled: Anticipation, Acceleration, and the Danish StateRikke Sand AndersenNoch keine Bewertungen
- Link JurnalDokument1 SeiteLink JurnalAdi PranataNoch keine Bewertungen
- Donovanosis (Granuloma Inguinale) : Part 2FDokument2 SeitenDonovanosis (Granuloma Inguinale) : Part 2FAdi PranataNoch keine Bewertungen
- Healthline: Prevalence of Skin Morbidity Among Construction Site Workers Working at VadodaraDokument3 SeitenHealthline: Prevalence of Skin Morbidity Among Construction Site Workers Working at VadodaraAdi PranataNoch keine Bewertungen
- Sinensis Linn) - Therefore, Research Is Needed To Determine The Effect of Extracts ofDokument1 SeiteSinensis Linn) - Therefore, Research Is Needed To Determine The Effect of Extracts ofAdi PranataNoch keine Bewertungen
- Penyuluhan Gizi Balita Di Posyandu Beng Kaja Kauh Upt Kesmas Gianyar IDokument1 SeitePenyuluhan Gizi Balita Di Posyandu Beng Kaja Kauh Upt Kesmas Gianyar IAdi PranataNoch keine Bewertungen
- Epigenetic Mechanisms From Gene To Protein A Complex Nonlinear and Eventful JourneyDokument5 SeitenEpigenetic Mechanisms From Gene To Protein A Complex Nonlinear and Eventful JourneyAdi PranataNoch keine Bewertungen
- Reference NewDokument2 SeitenReference NewAdi PranataNoch keine Bewertungen
- Micronutrients in Pregnancy: Robert E. BlackDokument5 SeitenMicronutrients in Pregnancy: Robert E. BlackAdi PranataNoch keine Bewertungen
- Differential Diagnosis of Retinopathy of Prematurity (ROP)Dokument1 SeiteDifferential Diagnosis of Retinopathy of Prematurity (ROP)Adi PranataNoch keine Bewertungen
- Learning Task 5Dokument1 SeiteLearning Task 5Adi PranataNoch keine Bewertungen
- HennaReviewProvisiona 2012lDokument22 SeitenHennaReviewProvisiona 2012lAdi PranataNoch keine Bewertungen
- Napoleon Lacroze Von Sanden - Crony Capitalism in ArgentinaDokument1 SeiteNapoleon Lacroze Von Sanden - Crony Capitalism in ArgentinaBoney LacrozeNoch keine Bewertungen
- Schedule 1 Allison Manufacturing Sales Budget For The Quarter I Ended March 31 First QuarterDokument16 SeitenSchedule 1 Allison Manufacturing Sales Budget For The Quarter I Ended March 31 First QuarterSultanz Farkhan SukmanaNoch keine Bewertungen
- Windows Server Failover Clustering On HPE SimpliVity Technical White Paper-A50000833enwDokument15 SeitenWindows Server Failover Clustering On HPE SimpliVity Technical White Paper-A50000833enwYeraldo MarinNoch keine Bewertungen
- Short Questions From 'The World Is Too Much With Us' by WordsworthDokument2 SeitenShort Questions From 'The World Is Too Much With Us' by WordsworthTANBIR RAHAMANNoch keine Bewertungen
- Indus River Valley Civilization ObjectivesDokument4 SeitenIndus River Valley Civilization ObjectivesArslan AsifNoch keine Bewertungen
- Jurisprudence Examination (Je) Information Guide: 5029-Reginfo - Je V2015.6.Docx Revised July 30, 2015Dokument10 SeitenJurisprudence Examination (Je) Information Guide: 5029-Reginfo - Je V2015.6.Docx Revised July 30, 2015yasahswi91Noch keine Bewertungen
- Managerial Accounting 14th Edition Warren Solutions Manual DownloadDokument28 SeitenManagerial Accounting 14th Edition Warren Solutions Manual DownloadRose Speers100% (22)
- Chapter 2: Related Theoretical Design Inputs 2.1 Sihwa Lake Tidal Power StationDokument9 SeitenChapter 2: Related Theoretical Design Inputs 2.1 Sihwa Lake Tidal Power Stationaldrin leeNoch keine Bewertungen
- The Impact of Eschatology and ProtologyDokument48 SeitenThe Impact of Eschatology and ProtologyJuan SteinNoch keine Bewertungen
- Class 11 Biology Notes Chapter 2 Studyguide360Dokument10 SeitenClass 11 Biology Notes Chapter 2 Studyguide360ANoch keine Bewertungen
- Formulating Affective Learning Targets: Category Examples and KeywordsDokument2 SeitenFormulating Affective Learning Targets: Category Examples and KeywordsJean LabradorNoch keine Bewertungen
- ch27 Matrices and ApplicationsDokument34 Seitench27 Matrices and Applicationschowa fellonNoch keine Bewertungen
- Economic and Product Design Considerations in MachiningDokument29 SeitenEconomic and Product Design Considerations in Machininghashir siddiquiNoch keine Bewertungen
- Question QP MCQ A BDokument60 SeitenQuestion QP MCQ A BPrashant JhaNoch keine Bewertungen
- DIN EN 16842-1: in Case of Doubt, The German-Language Original Shall Be Considered AuthoritativeDokument23 SeitenDIN EN 16842-1: in Case of Doubt, The German-Language Original Shall Be Considered AuthoritativeanupthattaNoch keine Bewertungen
- Rostam and SohrabDokument16 SeitenRostam and Sohrabronnel100% (1)
- Tazkira Mujaddid AlfesaniDokument53 SeitenTazkira Mujaddid AlfesanisayedNoch keine Bewertungen
- Kristen Tillett: ContactDokument2 SeitenKristen Tillett: ContactYtibNoch keine Bewertungen
- Odyssey Marine Exploration, Inc. v. The Unidentified, Shipwrecked Vessel or Vessels - Document No. 3Dokument11 SeitenOdyssey Marine Exploration, Inc. v. The Unidentified, Shipwrecked Vessel or Vessels - Document No. 3Justia.comNoch keine Bewertungen
- The Daily Jinx 0 - ENG-3 (1) - 1Dokument3 SeitenThe Daily Jinx 0 - ENG-3 (1) - 1NoxNoch keine Bewertungen
- Individual Assignment 1 (TPT630)Dokument7 SeitenIndividual Assignment 1 (TPT630)MUHAMMAD HABIB HARRAZ ABDUL RAHMANNoch keine Bewertungen
- Frontpage: Don'T Befriend Brutal DictatorsDokument16 SeitenFrontpage: Don'T Befriend Brutal DictatorsFrontPageAfricaNoch keine Bewertungen
- Text Al Capone B1Dokument2 SeitenText Al Capone B1Andjela JevremovicNoch keine Bewertungen
- Silent Reading With Graph1Dokument2 SeitenSilent Reading With Graph1JonaldSamueldaJoseNoch keine Bewertungen