Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Gynecology Notes Ebook PDFDokument51 SeitenGynecology Notes Ebook PDFThistell Thistle100% (1)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Polycystic Ovarian Syndrome (PCOS)Dokument10 SeitenPolycystic Ovarian Syndrome (PCOS)Juliet Amondi100% (1)
- PRP Slide PresentationDokument27 SeitenPRP Slide PresentationDrekka Hanibal Putra100% (5)
- OB-GYN Conceptual ExamDokument21 SeitenOB-GYN Conceptual Examquidditch07100% (5)
- Project Ease Biology Module 13Dokument30 SeitenProject Ease Biology Module 13Kebb Patrick Enar75% (4)
- Hormonal Cycle Lesson PlanDokument7 SeitenHormonal Cycle Lesson Plannisha kaushik100% (2)
- Progestogens in Obstetrics and Gynecology 2015th Edition (PRG)Dokument213 SeitenProgestogens in Obstetrics and Gynecology 2015th Edition (PRG)amenu_bizuneh100% (4)
- Gynecology Review: Abigail Elsie Dg. Castro, MD, Maed, Fpogs, Fpsuog August 11, 2017Dokument198 SeitenGynecology Review: Abigail Elsie Dg. Castro, MD, Maed, Fpogs, Fpsuog August 11, 2017Jojo Mendoza100% (1)
- Trans - Patten's Foundations of Embryology Chapters 1-7Dokument21 SeitenTrans - Patten's Foundations of Embryology Chapters 1-7Lorenzo Daniel Antonio0% (1)
- 7.recent Advances in Contraceptive TechnologyDokument25 Seiten7.recent Advances in Contraceptive TechnologyVeena Dalmeida100% (1)
- PDO Thread LiftsDokument2 SeitenPDO Thread LiftsDrekka Hanibal Putra33% (3)
- Vision Impairment: Prof. Sugana T, SPM (K)Dokument17 SeitenVision Impairment: Prof. Sugana T, SPM (K)Drekka Hanibal PutraNoch keine Bewertungen
- Abstract2 53648866Dokument1 SeiteAbstract2 53648866Drekka Hanibal PutraNoch keine Bewertungen
- Article3 12770175Dokument9 SeitenArticle3 12770175Drekka Hanibal PutraNoch keine Bewertungen
- RefraksiDokument53 SeitenRefraksigilaliNoch keine Bewertungen
- Amsler Grid Test Untuk ARMDDokument2 SeitenAmsler Grid Test Untuk ARMDDrekka Hanibal PutraNoch keine Bewertungen
- Article3 12770175Dokument9 SeitenArticle3 12770175Drekka Hanibal PutraNoch keine Bewertungen
- Article3 12770175Dokument9 SeitenArticle3 12770175Drekka Hanibal PutraNoch keine Bewertungen
- Auto Loge LDF Prospective Trial Ow MDokument17 SeitenAuto Loge LDF Prospective Trial Ow MDrekka Hanibal PutraNoch keine Bewertungen
- Platelet-Rich Plasma Enhances The Initial Mobilization of Circulation-Derived Cells For Tendon HealingDokument3 SeitenPlatelet-Rich Plasma Enhances The Initial Mobilization of Circulation-Derived Cells For Tendon HealingDrekka Hanibal PutraNoch keine Bewertungen
- PRP Haarausfall EnglischDokument5 SeitenPRP Haarausfall EnglischDrekka Hanibal PutraNoch keine Bewertungen
- Article4 64101236Dokument2 SeitenArticle4 64101236Drekka Hanibal PutraNoch keine Bewertungen
- Zenker 92749841Dokument8 SeitenZenker 92749841Drekka Hanibal PutraNoch keine Bewertungen
- M - LiftingDokument2 SeitenM - LiftingDrekka Hanibal PutraNoch keine Bewertungen
- Higher Cortisol Level Would Increase The Risk of Spontaneous AbortionDokument8 SeitenHigher Cortisol Level Would Increase The Risk of Spontaneous AbortionDrekka Hanibal PutraNoch keine Bewertungen
- Abstract2 53648866Dokument1 SeiteAbstract2 53648866Drekka Hanibal PutraNoch keine Bewertungen
- Higher Cortisol Level Would Increase The Risk of Spontaneous AbortionDokument8 SeitenHigher Cortisol Level Would Increase The Risk of Spontaneous AbortionDrekka Hanibal PutraNoch keine Bewertungen
- Higher Cortisol Level Would Increase The Risk of Spontaneous AbortionDokument8 SeitenHigher Cortisol Level Would Increase The Risk of Spontaneous AbortionDrekka Hanibal PutraNoch keine Bewertungen
- Calcium (Umum)Dokument13 SeitenCalcium (Umum)Drekka Hanibal PutraNoch keine Bewertungen
- Higher Cortisol Level Would Increase The Risk of Spontaneous AbortionDokument8 SeitenHigher Cortisol Level Would Increase The Risk of Spontaneous AbortionDrekka Hanibal PutraNoch keine Bewertungen
- 3836 7224 1 SMDokument10 Seiten3836 7224 1 SMMade Ayu Sukma AsrityaNoch keine Bewertungen
- Alcium in Regnancy and Actation: Ann PrenticeDokument26 SeitenAlcium in Regnancy and Actation: Ann PrenticeDrekka Hanibal PutraNoch keine Bewertungen
- Alcium in Regnancy and Actation: Ann PrenticeDokument26 SeitenAlcium in Regnancy and Actation: Ann PrenticeDrekka Hanibal PutraNoch keine Bewertungen
- Higher Cortisol Level Would Increase The Risk of Spontaneous AbortionDokument8 SeitenHigher Cortisol Level Would Increase The Risk of Spontaneous AbortionDrekka Hanibal PutraNoch keine Bewertungen
- 1369 1482 1 PBDokument4 Seiten1369 1482 1 PBDrekka Hanibal PutraNoch keine Bewertungen
- 3836 7224 1 SMDokument10 Seiten3836 7224 1 SMMade Ayu Sukma AsrityaNoch keine Bewertungen
- Nej Mic M 1111814Dokument1 SeiteNej Mic M 1111814Drekka Hanibal PutraNoch keine Bewertungen
- Meditation For The Womens MonthDokument4 SeitenMeditation For The Womens Monthsanja9balerNoch keine Bewertungen
- Sexuality and Its Disorders Development Cases and Treatment 1St Edition Abrams Test Bank Full Chapter PDFDokument27 SeitenSexuality and Its Disorders Development Cases and Treatment 1St Edition Abrams Test Bank Full Chapter PDFkhaidu00drxn100% (9)
- Hormones and The Menstrual Cycle: Discussion GuideDokument11 SeitenHormones and The Menstrual Cycle: Discussion GuideJohnryl FranciscoNoch keine Bewertungen
- Jss1 Basic Science 3rd TermDokument2 SeitenJss1 Basic Science 3rd Term0yewale mustaphaNoch keine Bewertungen
- Chapt 27 Ap2Dokument5 SeitenChapt 27 Ap2candybio83Noch keine Bewertungen
- Week 5 Study GuideDokument12 SeitenWeek 5 Study GuideSneha PatelNoch keine Bewertungen
- 2 Study of Female Pelvic Pain ..Dokument69 Seiten2 Study of Female Pelvic Pain ..Ghofran Ibrahim HassanNoch keine Bewertungen
- DLL November 21, 2017 - Endocrine GlandsDokument4 SeitenDLL November 21, 2017 - Endocrine GlandsHelen Grace Llemos Cabalag100% (2)
- Inmuno 555Dokument11 SeitenInmuno 555Daniela Fdz CNoch keine Bewertungen
- Cblebypu 02Dokument8 SeitenCblebypu 02Rizwan AliNoch keine Bewertungen
- Test PaperDokument4 SeitenTest PaperKimberley TadeoNoch keine Bewertungen
- ObGyn Board Review PDFDokument85 SeitenObGyn Board Review PDFCoolrobertizNoch keine Bewertungen
- 2.animal Reprodcation and Developmental BiologyDokument88 Seiten2.animal Reprodcation and Developmental BiologyAnkit JyaniNoch keine Bewertungen
- The Endocrinopathies of Anorexia NervosaDokument13 SeitenThe Endocrinopathies of Anorexia NervosaCarla MesquitaNoch keine Bewertungen
- AMENORRHOEADokument16 SeitenAMENORRHOEAĶHwola ƏľsHokryNoch keine Bewertungen
- Menstrual Hygiene Amongst The School Going Adolescent Girls in Rural AreaDokument5 SeitenMenstrual Hygiene Amongst The School Going Adolescent Girls in Rural AreaMuhammad GhiffariNoch keine Bewertungen
- Revision - Test - Topic - 7 - To - 17 MsDokument33 SeitenRevision - Test - Topic - 7 - To - 17 MsZaigham ZiaNoch keine Bewertungen
- Menstrual Cycle QuizDokument2 SeitenMenstrual Cycle QuizPalwasha Khan100% (1)
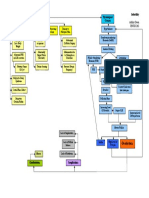
- Infertility Concept MapDokument1 SeiteInfertility Concept Mapashleydean0% (1)
- Imams Gynac Mahima July2011Dokument92 SeitenImams Gynac Mahima July2011Pallavi PatilNoch keine Bewertungen
- AIPMT Sample Paper-6 (2009-Sample Paper)Dokument50 SeitenAIPMT Sample Paper-6 (2009-Sample Paper)Firdosh Khan100% (1)