Das könnte Ihnen auch gefallen
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Von EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Bewertung: 5 von 5 Sternen5/5 (4)
- Study Checklist For Passing NCLEX-RN - AllnursesDokument2 SeitenStudy Checklist For Passing NCLEX-RN - AllnursesbeingfiredNoch keine Bewertungen
- NCLEX Study GuideDokument2 SeitenNCLEX Study GuideLogin Nurse100% (1)
- Nclex 3500Dokument4 SeitenNclex 3500chitorNoch keine Bewertungen
- NCLEXDokument3 SeitenNCLEXKath Cuevas50% (2)
- NCLEXDokument27 SeitenNCLEXMary Hope A. Lima100% (1)
- The Client Should Be Instructed As Follows: Intravenous Pyelogram (IVP) Is An X-Ray of The Urinary SystemDokument25 SeitenThe Client Should Be Instructed As Follows: Intravenous Pyelogram (IVP) Is An X-Ray of The Urinary SystemElizabeth SharmaNoch keine Bewertungen
- Nclex-Rn Test Study GuideDokument199 SeitenNclex-Rn Test Study GuideSusan BensonNoch keine Bewertungen
- Random NCLEX Tips 101 AileenDokument9 SeitenRandom NCLEX Tips 101 AileenxaileenxNoch keine Bewertungen
- Nclex Study GuideDokument35 SeitenNclex Study Guideapi-238869635100% (3)
- NCSBN - Pharmacology and ParenteralDokument36 SeitenNCSBN - Pharmacology and ParenteralKarissa May Cortez92% (12)
- Mark K Lecture #2Dokument16 SeitenMark K Lecture #2Melissa Sapp100% (2)
- Nurse collecting data on acute MI findingsDokument6 SeitenNurse collecting data on acute MI findingsNadim Khalid0% (1)
- Nclex TipsDokument23 SeitenNclex TipsYA HO100% (2)
- Crutch Walking Techniques and Safety TipsDokument2 SeitenCrutch Walking Techniques and Safety Tipsjanet rooseveltNoch keine Bewertungen
- Nclex PointersDokument2 SeitenNclex PointersKira95% (19)
- My Nclex Study GuideDokument4 SeitenMy Nclex Study GuideLogin Nurse100% (1)
- Nclex HelpDokument18 SeitenNclex HelpHumbe OshunNoch keine Bewertungen
- NCLEX questions on medications and pharmacologyDokument82 SeitenNCLEX questions on medications and pharmacologyMaria Nadia Mihalik100% (3)
- Calcium, seizures, nephrotoxicity, hypertension, infection, tremors hirsutismDokument18 SeitenCalcium, seizures, nephrotoxicity, hypertension, infection, tremors hirsutismmaane1005Noch keine Bewertungen
- NCLEX2015Dokument61 SeitenNCLEX2015Sara Pirman100% (2)
- NCLEX Study GuideDokument7 SeitenNCLEX Study Guidemmgoodall22100% (3)
- Mind Web Academy - Booster 3Dokument8 SeitenMind Web Academy - Booster 3Charis Gutierrez RodriguezNoch keine Bewertungen
- Delegation NCLEX-RNDokument3 SeitenDelegation NCLEX-RNPrince K. Tailey100% (1)
- NCLEX Study GuideDokument35 SeitenNCLEX Study Guidedchirinos90100% (1)
- Nclex GuideDokument3 SeitenNclex Guidemichegirl91Noch keine Bewertungen
- Nclex Random Fact To StudyDokument431 SeitenNclex Random Fact To StudyNeko Neko100% (1)
- NCLEX Tips On ProceduresDokument4 SeitenNCLEX Tips On Proceduresromin_soledad100% (7)
- The Nclex-Pn Cram Sheet: General Test Information Normal Lab ValuesDokument2 SeitenThe Nclex-Pn Cram Sheet: General Test Information Normal Lab Valuesroboat96Noch keine Bewertungen
- NCLEXDokument95 SeitenNCLEXKurt Sturgeon67% (3)
- Select All That Apply SATADokument58 SeitenSelect All That Apply SATANicholas TagleNoch keine Bewertungen
- Testing - 2 NclexDokument12 SeitenTesting - 2 NclexYoke W KhooNoch keine Bewertungen
- Key Concepts For An NCLEX-RN Cram SheetDokument3 SeitenKey Concepts For An NCLEX-RN Cram Sheetema100% (2)
- Every Monday in May Live Facebook ReviewDokument4 SeitenEvery Monday in May Live Facebook ReviewChelle RocoNoch keine Bewertungen
- Cardiovascular Summary Saunders Comprehensive Review For The Nclex RN ExaminationDokument40 SeitenCardiovascular Summary Saunders Comprehensive Review For The Nclex RN ExaminationdanicaNoch keine Bewertungen
- NCLEX FundamentalsDokument13 SeitenNCLEX FundamentalsSara Pirman100% (1)
- Nclex 2Dokument147 SeitenNclex 2Habet Fidem100% (5)
- My Pledge My NCLEX Success PlanDokument2 SeitenMy Pledge My NCLEX Success PlanAnjali Naudiyal100% (1)
- P and D Study GuideDokument4 SeitenP and D Study GuideKenneth Smith II100% (1)
- NCLEXDokument3 SeitenNCLEXEternity RealNoch keine Bewertungen
- Day Complete GuideDokument25 SeitenDay Complete GuideWillie Melono Nkolo100% (1)
- Delegation To LPN & Nap: Prepared byDokument7 SeitenDelegation To LPN & Nap: Prepared byJamilla louise Valencia100% (1)
- NGN Workbook PDFDokument11 SeitenNGN Workbook PDFramandeep kaurNoch keine Bewertungen
- Nclex Cheat SheetDokument9 SeitenNclex Cheat Sheetsophia onuNoch keine Bewertungen
- Strategy DefinitionsDokument8 SeitenStrategy DefinitionskwameNoch keine Bewertungen
- Nclex-Rn Essential Questions and RationalesDokument96 SeitenNclex-Rn Essential Questions and RationalesGloryJane100% (1)
- NCLEX Select All That Apply Practice Exam QuestionsDokument67 SeitenNCLEX Select All That Apply Practice Exam QuestionsHermie Joy Maglaqui100% (1)
- 115-NCLEX-RN Review Made Incredibly Easy, Fifth Edition (Incredibly Easy Series) - Lippincott-16083 - p36Dokument1 Seite115-NCLEX-RN Review Made Incredibly Easy, Fifth Edition (Incredibly Easy Series) - Lippincott-16083 - p36MuhNatsirNoch keine Bewertungen
- NCLEX Review: Essential Concepts for SuccessDokument11 SeitenNCLEX Review: Essential Concepts for SuccessNaidin Catherine De Guzman-AlcalaNoch keine Bewertungen
- Med Surge 2 Mod 1 CardiacDokument13 SeitenMed Surge 2 Mod 1 CardiacDirk Buckner100% (2)
- 1430 Drug CardsfinalDokument7 Seiten1430 Drug CardsfinalLizSherman100% (1)
- Vitamin K IV antidote for warfarin bleedingDokument10 SeitenVitamin K IV antidote for warfarin bleedingQueennitaNoch keine Bewertungen
- Mental Health Nclex High YieldDokument32 SeitenMental Health Nclex High Yieldnene lewis100% (1)
- NCLEX Seminar ManuscriptDokument53 SeitenNCLEX Seminar ManuscriptKim Medairos100% (1)
- Hesi HintsDokument42 SeitenHesi HintsJohn Thomas100% (2)
- Nclex Exam PrepDokument26 SeitenNclex Exam PrepPascal St Peter Nwaorgu100% (1)
- Essential care considerations for common pediatric and medical conditionsDokument97 SeitenEssential care considerations for common pediatric and medical conditionsMary Aurine FullanteNoch keine Bewertungen
- NCLEX-by SUKAWINACADokument44 SeitenNCLEX-by SUKAWINACAAri WijayantiNoch keine Bewertungen
- Nclex RN MedsDokument16 SeitenNclex RN MedsAli ResendizNoch keine Bewertungen
- King Rush MoreDokument1 SeiteKing Rush MoreawuahbohNoch keine Bewertungen
- Oop Say You Know MeDokument1 SeiteOop Say You Know MeawuahbohNoch keine Bewertungen
- Pharm NclexDokument9 SeitenPharm NclexawuahbohNoch keine Bewertungen
- Article For CET CHFDokument5 SeitenArticle For CET CHFawuahbohNoch keine Bewertungen
- Article For JournalDokument6 SeitenArticle For JournalawuahbohNoch keine Bewertungen
- PolypharmacyDokument24 SeitenPolypharmacySurina Zaman HuriNoch keine Bewertungen
- HandOff SampleToolsDokument9 SeitenHandOff SampleToolsOllie EvansNoch keine Bewertungen
- The BSN Job Search: Interview Preparation: Telling Your StoryDokument25 SeitenThe BSN Job Search: Interview Preparation: Telling Your StoryawuahbohNoch keine Bewertungen
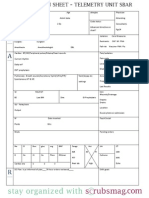
- Nurse Brain Sheet Telemetry Unit SBARDokument1 SeiteNurse Brain Sheet Telemetry Unit SBARvsosa624Noch keine Bewertungen
- NCLEX Random FactsDokument34 SeitenNCLEX Random FactsLegnaMary100% (8)
- Probability of A or B and A and B-1Dokument2 SeitenProbability of A or B and A and B-1awuahbohNoch keine Bewertungen
- Middle Age Adult Health History Assignment Guidelines N315 Fall 2013Dokument23 SeitenMiddle Age Adult Health History Assignment Guidelines N315 Fall 2013awuahbohNoch keine Bewertungen
- EBP Article 1Dokument11 SeitenEBP Article 1awuahbohNoch keine Bewertungen
- Massachusetts Department of Public HealthDokument24 SeitenMassachusetts Department of Public HealthawuahbohNoch keine Bewertungen
- Tips On Answering NclexDokument4 SeitenTips On Answering NclexawuahbohNoch keine Bewertungen
- EBP Article 3Dokument6 SeitenEBP Article 3awuahbohNoch keine Bewertungen
- Critical Thinking StrategiesDokument3 SeitenCritical Thinking StrategiesawuahbohNoch keine Bewertungen
- Random FactsDokument338 SeitenRandom Factscyram81100% (1)
- Therapeutic CommunicationDokument1 SeiteTherapeutic CommunicationawuahbohNoch keine Bewertungen
- ENT Throat and EsophagusDokument41 SeitenENT Throat and EsophagusMUHAMMAD HASAN NAGRANoch keine Bewertungen
- Article For CET CHFDokument5 SeitenArticle For CET CHFawuahbohNoch keine Bewertungen
- STDA VaricealDokument8 SeitenSTDA VaricealDeisy de JesusNoch keine Bewertungen
- Parkland formula and rule of 9Dokument8 SeitenParkland formula and rule of 9awuahbohNoch keine Bewertungen
- Patient Report FormDokument1 SeitePatient Report FormawuahbohNoch keine Bewertungen
- Debate 3 Youth Incarceration in Adult PrisonsDokument6 SeitenDebate 3 Youth Incarceration in Adult PrisonsawuahbohNoch keine Bewertungen
- Article For Jouranal 2 (498P)Dokument5 SeitenArticle For Jouranal 2 (498P)awuahbohNoch keine Bewertungen
- Does Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorDokument24 SeitenDoes Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorawuahbohNoch keine Bewertungen
- Article For Journal 4-18-14Dokument8 SeitenArticle For Journal 4-18-14awuahbohNoch keine Bewertungen
- Article For JournalDokument6 SeitenArticle For JournalawuahbohNoch keine Bewertungen
- Related Links: Cholestyramine ColestipolDokument2 SeitenRelated Links: Cholestyramine ColestipolJireh Mae CorderoNoch keine Bewertungen
- M 3Dokument10 SeitenM 3Aijem RyanNoch keine Bewertungen
- Nursing Management of HypertensionDokument9 SeitenNursing Management of HypertensionsarasjunkNoch keine Bewertungen
- Natural Medicines Comprehensive Database 2010Dokument26 SeitenNatural Medicines Comprehensive Database 2010PsineticNoch keine Bewertungen
- Medical-Surgical Nursing Lecture NotesDokument90 SeitenMedical-Surgical Nursing Lecture NotesJessica AnisNoch keine Bewertungen
- FLASHCARD CardiovascularDokument40 SeitenFLASHCARD CardiovascularsnehaNoch keine Bewertungen
- 2 6 7 HypervolemiaDokument4 Seiten2 6 7 HypervolemiaMaica LectanaNoch keine Bewertungen
- DOSES FOR SMALL ANIMALS: KEY MEDICATIONS FOR RABBITS, RODENTS, REPTILES AND BIRDSDokument14 SeitenDOSES FOR SMALL ANIMALS: KEY MEDICATIONS FOR RABBITS, RODENTS, REPTILES AND BIRDSBruna MoreiraNoch keine Bewertungen
- Critical Care MedsDokument3 SeitenCritical Care MedsAlyssa Newsome NixonNoch keine Bewertungen
- Cardiovascular Drugs and the Renin-Angiotensin SystemDokument16 SeitenCardiovascular Drugs and the Renin-Angiotensin SystemAngel DiangNoch keine Bewertungen
- "Natural Healing With Herbs For A Healthier You": DandelionDokument5 Seiten"Natural Healing With Herbs For A Healthier You": Dandelionak09100% (1)
- Aminoglycoside Toxicity and NephrotoxicityDokument47 SeitenAminoglycoside Toxicity and NephrotoxicityAimee Gutierrez91% (55)
- Case Presentation On Systemic Lupus Erythematosus (SLE) : Presented By: Mahitha Karimsetti 616175802018 Pharm. D InternDokument35 SeitenCase Presentation On Systemic Lupus Erythematosus (SLE) : Presented By: Mahitha Karimsetti 616175802018 Pharm. D Internsrija vijjapuNoch keine Bewertungen
- Emergency DrugsDokument15 SeitenEmergency Drugsjheverly123100% (1)
- X. Medical ManagementDokument12 SeitenX. Medical ManagementXy-Za Roy MarieNoch keine Bewertungen
- FurosemideDokument4 SeitenFurosemideapi-3797941100% (1)
- Mata Drug Study FurosemideDokument14 SeitenMata Drug Study FurosemideNicole Keesha MataNoch keine Bewertungen
- Case Study Orientation SlidesDokument88 SeitenCase Study Orientation SlidesJoseph Emmanuel CandaNoch keine Bewertungen
- Heart Failure AssignmentDokument6 SeitenHeart Failure AssignmentclarheenaNoch keine Bewertungen
- 10.1007@s10157 020 01867 yDokument6 Seiten10.1007@s10157 020 01867 yGin RummyNoch keine Bewertungen
- April 20, 2015 - RATIODokument23 SeitenApril 20, 2015 - RATIOLouie BelloNoch keine Bewertungen
- Name of The Experiment: Evaluation of CNS Activity of Diazepam On Mice. Principle: ApparatusDokument8 SeitenName of The Experiment: Evaluation of CNS Activity of Diazepam On Mice. Principle: Apparatusdipto kumer sarkerNoch keine Bewertungen
- USNI Medication TestDokument8 SeitenUSNI Medication Testusni100% (31)
- Obat Paketan OKDokument3 SeitenObat Paketan OKDiana AuliaNoch keine Bewertungen
- Online IVDrugChartDokument23 SeitenOnline IVDrugChartKenneth Remolete100% (1)
- Drug Study On Emergency DrugsDokument14 SeitenDrug Study On Emergency DrugsRene John FranciscoNoch keine Bewertungen
- Diuretics - AMBOSS PDFDokument9 SeitenDiuretics - AMBOSS PDFOpio Isaac100% (1)
- NCP and DSDokument6 SeitenNCP and DSfranzcatchie100% (1)
- Question Bank PT-II SET 02 Question Paper 2021Dokument20 SeitenQuestion Bank PT-II SET 02 Question Paper 2021xyzNoch keine Bewertungen
- Pharmacology Practice Test IDokument27 SeitenPharmacology Practice Test Isidharta_chatterjeeNoch keine Bewertungen