Das könnte Ihnen auch gefallen
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicVon EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicBewertung: 5 von 5 Sternen5/5 (1)
- Problem # 2: Uncontrolled HypertensionDokument5 SeitenProblem # 2: Uncontrolled HypertensionGlydenne GayamNoch keine Bewertungen
- Physical Exam Template FormatDokument2 SeitenPhysical Exam Template Formatbladimer_ria100% (1)
- Acute AppendicitisDokument14 SeitenAcute AppendicitisJane GarciaNoch keine Bewertungen
- Guide in Reporting Complete Physical Examination (2013) - Source: Bates' Guide To Physical Examination.Dokument8 SeitenGuide in Reporting Complete Physical Examination (2013) - Source: Bates' Guide To Physical Examination.Ernie G. Bautista II, RN, MD100% (6)
- 3 RosDokument11 Seiten3 RosShereen AlobinayNoch keine Bewertungen
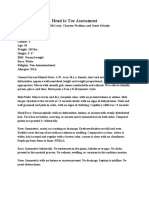
- Weebly Head To Toe AssessmentDokument3 SeitenWeebly Head To Toe Assessmentapi-608265381Noch keine Bewertungen
- Case Presentation CUPDokument42 SeitenCase Presentation CUPAshokNoch keine Bewertungen
- Sample POMRDokument4 SeitenSample POMRJeffrey RamosNoch keine Bewertungen
- Dolinta, Josephine L.: Clinical Paper Pediatric WardDokument10 SeitenDolinta, Josephine L.: Clinical Paper Pediatric WardAnonymous JlE9AygNoch keine Bewertungen
- AbortionDokument16 SeitenAbortionKim Lompot100% (1)
- SURGERY Hemorrhoids PEDokument3 SeitenSURGERY Hemorrhoids PEJim Christian EllaserNoch keine Bewertungen
- COPD Final PPT SiddyDokument124 SeitenCOPD Final PPT SiddySid FlavierNoch keine Bewertungen
- Care Paln For HypetensionDokument21 SeitenCare Paln For Hypetensionlanguha NgatiNoch keine Bewertungen
- Case 1Dokument60 SeitenCase 1senny chapagainNoch keine Bewertungen
- Case Write Up 1Dokument8 SeitenCase Write Up 1Mohammed AlshehriNoch keine Bewertungen
- Normal PEDokument5 SeitenNormal PEFray BotodNoch keine Bewertungen
- Case PresentationDokument41 SeitenCase PresentationAhmad NawazNoch keine Bewertungen
- CASE REPORT Neurosurgery2 For CraniopharyngiomaDokument7 SeitenCASE REPORT Neurosurgery2 For CraniopharyngiomaIcekung KasamepongtongdeeNoch keine Bewertungen
- Physical ExaminationDokument3 SeitenPhysical ExaminationAlexandra Duque-DavidNoch keine Bewertungen
- Physical Assessment PDFDokument8 SeitenPhysical Assessment PDFsunshine jeonNoch keine Bewertungen
- Sample POMRDokument4 SeitenSample POMRJeffrey RamosNoch keine Bewertungen
- Case Report - CC - Uraemic EncephalopathyDokument11 SeitenCase Report - CC - Uraemic EncephalopathyM CubedNoch keine Bewertungen
- PEDokument34 SeitenPEbrigette_lagatNoch keine Bewertungen
- Physical Examination PediaDokument2 SeitenPhysical Examination PediaNorman jOyeNoch keine Bewertungen
- Physical Exam Write Up IdealDokument2 SeitenPhysical Exam Write Up Idealsintwala0% (1)
- ROS FinalDokument1 SeiteROS FinaldaleascabanoNoch keine Bewertungen
- 11 - Dot Phrase Templates HMC ED June 2017 - Rev 9.6.17Dokument13 Seiten11 - Dot Phrase Templates HMC ED June 2017 - Rev 9.6.17M100% (1)
- SOAP TempDokument2 SeitenSOAP TempwestplatteNoch keine Bewertungen
- Pedia Ward HXDokument4 SeitenPedia Ward HXMalshika JayatissaNoch keine Bewertungen
- Pediatric Pe - TdcedenoDokument4 SeitenPediatric Pe - TdcedenoDenise CedeñoNoch keine Bewertungen
- Soap Note Week 5Dokument11 SeitenSoap Note Week 5Robert AgumbaNoch keine Bewertungen
- Case Study TpapnDokument7 SeitenCase Study TpapnAnjali NaudiyalNoch keine Bewertungen
- Derma Case Write UpDokument9 SeitenDerma Case Write UpAmbhi GanaNoch keine Bewertungen
- SABER-Nursing Care Plan #1 - JGDokument7 SeitenSABER-Nursing Care Plan #1 - JGJessica MontoyaNoch keine Bewertungen
- Anp Case Presentation of Icu 103 Sem IiDokument26 SeitenAnp Case Presentation of Icu 103 Sem IiShilpa JoshiNoch keine Bewertungen
- Final Physical ExaminationDokument3 SeitenFinal Physical Examinationapi-620159117Noch keine Bewertungen
- Conradi Hünermann SyndromeDokument12 SeitenConradi Hünermann Syndromejoerobinson8889323Noch keine Bewertungen
- Congenital HypothyroidismDokument10 SeitenCongenital HypothyroidismEmily EresumaNoch keine Bewertungen
- Case Protocol - GBS - TanguilanDokument7 SeitenCase Protocol - GBS - TanguilanRosealie TanguilanNoch keine Bewertungen
- Nephrotic SyndromeDokument61 SeitenNephrotic SyndromeRanah Julia Garchitorena AyoNoch keine Bewertungen
- Physical Examination ChildDokument2 SeitenPhysical Examination Childwydiake3Noch keine Bewertungen
- AhafinalheadtoeDokument4 SeitenAhafinalheadtoeapi-620081868Noch keine Bewertungen
- Soft TIssue LesionDokument15 SeitenSoft TIssue LesionQp NizamNoch keine Bewertungen
- Covid-19 CaseDokument9 SeitenCovid-19 CaseKartik SharmaNoch keine Bewertungen
- Cebu Doctors' University Department of Internal Medicine EndorsementDokument38 SeitenCebu Doctors' University Department of Internal Medicine EndorsementRalph de la TorreNoch keine Bewertungen
- Screenshot 2023-02-19 at 11.11.49 AMDokument24 SeitenScreenshot 2023-02-19 at 11.11.49 AMabdulrahmanNoch keine Bewertungen
- Easter College: Department of NursingDokument13 SeitenEaster College: Department of NursingShaii shanNoch keine Bewertungen
- Hashim Major LogDokument26 SeitenHashim Major LogHashim AlsammawiNoch keine Bewertungen
- Breast and Endocrine Case Report - Mohammed AlrubaiaanDokument8 SeitenBreast and Endocrine Case Report - Mohammed Alrubaiaantwgp6pg5ghNoch keine Bewertungen
- Ent Case Report Acute Otitis Media Stage IIIDokument12 SeitenEnt Case Report Acute Otitis Media Stage IIIRem Alfelor100% (1)
- Module 4 Soap NoteDokument5 SeitenModule 4 Soap Noteapi-539434803Noch keine Bewertungen
- Long Case Presentation: Saadia Rehman (1502-mbbs-038)Dokument42 SeitenLong Case Presentation: Saadia Rehman (1502-mbbs-038)Radial ArteryNoch keine Bewertungen
- Dermato CHDokument10 SeitenDermato CHSuthan KaveriNoch keine Bewertungen
- Case Report: Division ADokument19 SeitenCase Report: Division AAyuub AbdirizakNoch keine Bewertungen
- Team C Final Written OutputDokument22 SeitenTeam C Final Written OutputCarina SuarezNoch keine Bewertungen
- Medex Exam Writeups PageDokument9 SeitenMedex Exam Writeups Pageaahmad87Noch keine Bewertungen
- Physical ExamDokument3 SeitenPhysical ExamMaddi AlonzoNoch keine Bewertungen
- N174 Physical Assessment-Final Study GuideDokument14 SeitenN174 Physical Assessment-Final Study GuideMark Angelo Picar AbelleraNoch keine Bewertungen
- Medical Report - PneumoniaeDokument8 SeitenMedical Report - Pneumoniaenguyenhoavanchi2002Noch keine Bewertungen
- Trauma Resident Manual 2022Dokument37 SeitenTrauma Resident Manual 2022jhk0428Noch keine Bewertungen
- 2023.04.19 - CPC PresentationDokument20 Seiten2023.04.19 - CPC Presentationjhk0428Noch keine Bewertungen
- Pulmonary EmbolismDokument61 SeitenPulmonary Embolismjhk0428Noch keine Bewertungen
- Step 3 NotesDokument4 SeitenStep 3 Notesjhk0428Noch keine Bewertungen
- Superior Vena Cava Obstruction: Aditya Rachakonda, PGY4 December 8, 2014Dokument35 SeitenSuperior Vena Cava Obstruction: Aditya Rachakonda, PGY4 December 8, 2014jhk0428Noch keine Bewertungen
- Vqi - HDDokument2 SeitenVqi - HDjhk0428Noch keine Bewertungen
- Thoracic and Abdominal TraumaDokument76 SeitenThoracic and Abdominal Traumajhk0428100% (1)
- VESAP 4 NotesDokument63 SeitenVESAP 4 Notesjhk0428100% (1)
- Debate Tibial Percutaneous Interventions DESDokument37 SeitenDebate Tibial Percutaneous Interventions DESjhk0428Noch keine Bewertungen
- VESAP Study Guide 2Dokument8 SeitenVESAP Study Guide 2jhk0428Noch keine Bewertungen
- Aorto Iliac DiseaseDokument58 SeitenAorto Iliac Diseasejhk0428100% (1)
- VESAP Study GuideDokument5 SeitenVESAP Study Guidejhk0428Noch keine Bewertungen
- 3 Session 3 - AbdominalExamDokument15 Seiten3 Session 3 - AbdominalExamjhk0428Noch keine Bewertungen
- Mini-CPX 6 Part 1 - HistoryDokument6 SeitenMini-CPX 6 Part 1 - Historyjhk0428Noch keine Bewertungen
- Health Literacy Seminar Effective StoryDokument2 SeitenHealth Literacy Seminar Effective Storyjhk0428Noch keine Bewertungen
- 2015 07 08 Case PresentationDokument12 Seiten2015 07 08 Case Presentationjhk0428Noch keine Bewertungen
- 15-05-29 TBTC Soap NoteDokument2 Seiten15-05-29 TBTC Soap Notejhk0428Noch keine Bewertungen
- Mini-CPX 6 Part 2 - Physical ExamDokument7 SeitenMini-CPX 6 Part 2 - Physical Examjhk0428Noch keine Bewertungen
- Renal Histology Biolucida AnswersDokument6 SeitenRenal Histology Biolucida Answersjhk0428Noch keine Bewertungen
- Disease Cheat SheetDokument393 SeitenDisease Cheat Sheetjhk0428100% (1)
- American Council On Science and Health - Meet Your New Organ - The Mesentery - 2017-02-17Dokument3 SeitenAmerican Council On Science and Health - Meet Your New Organ - The Mesentery - 2017-02-17RovanNoch keine Bewertungen
- Shouldice HospitalDokument5 SeitenShouldice HospitalBibhutesh NayakNoch keine Bewertungen
- Hospital Requirement-FinalDokument9 SeitenHospital Requirement-FinalPrasanna Ramasamy100% (1)
- Morning Report PSPDokument9 SeitenMorning Report PSPJessicaNoch keine Bewertungen
- Personal and Educational Informatics Assignment (Skyla Fiesta)Dokument2 SeitenPersonal and Educational Informatics Assignment (Skyla Fiesta)Skyla FiestaNoch keine Bewertungen
- 1 RMNCHA StrategyDokument83 Seiten1 RMNCHA StrategyDivyaDeepthi18Noch keine Bewertungen
- Vaginal Exam Learning GuideDokument2 SeitenVaginal Exam Learning GuideAprilian Ayu SitaNoch keine Bewertungen
- ISUOG Lecture-5-Informed-consent-image-recording-report-writing-ACDokument34 SeitenISUOG Lecture-5-Informed-consent-image-recording-report-writing-ACTansya PurnaningrumNoch keine Bewertungen
- 7-Week Usmle Step 1 Sample ScheduleDokument2 Seiten7-Week Usmle Step 1 Sample ScheduleHannah ChanNoch keine Bewertungen
- DPH Governor General Programme 2017 FinalDokument6 SeitenDPH Governor General Programme 2017 Finalterry johnsonNoch keine Bewertungen
- Valores Referencias AIA - TosohDokument4 SeitenValores Referencias AIA - TosohZelene Cordova Roman100% (1)
- Collated Thyroid PBLDokument13 SeitenCollated Thyroid PBLnik_khadijah_2Noch keine Bewertungen
- Electrical in Medical LocationDokument32 SeitenElectrical in Medical LocationengrrafNoch keine Bewertungen
- Management of Patients With Female Reproductive Disorders: Ance M. SiallaganDokument40 SeitenManagement of Patients With Female Reproductive Disorders: Ance M. SiallagananchemeysNoch keine Bewertungen
- An Introduction To Spanish For Health Care Workers Communication and Culture Third EditionDokument398 SeitenAn Introduction To Spanish For Health Care Workers Communication and Culture Third EditionSewist YUL100% (7)
- Fast Hugs MaidenDokument8 SeitenFast Hugs MaidenPriscila Navarro MedinaNoch keine Bewertungen
- Rubella and PregnancyDokument6 SeitenRubella and PregnancyKABERA RENENoch keine Bewertungen
- Summary of Purposes and ObjectivesDokument19 SeitenSummary of Purposes and Objectivesrodolfo opido100% (1)
- Mendelson Syndrome - StatPearls - NCBI BookshelfDokument8 SeitenMendelson Syndrome - StatPearls - NCBI Bookshelfcesar aNoch keine Bewertungen
- Zeller 2004Dokument6 SeitenZeller 2004Riany Jade SabrinaNoch keine Bewertungen
- Total ProteinDokument3 SeitenTotal ProteinTriRatnaFauziah50% (2)
- GKNM Hospital ReportDokument33 SeitenGKNM Hospital ReportKarthi KeyanNoch keine Bewertungen
- Vascular Access Principles and Practice by Samuel Eric WilsonDokument328 SeitenVascular Access Principles and Practice by Samuel Eric WilsonBruno ZanuttiniNoch keine Bewertungen
- A. KMC Introduction, Components & BenefitsDokument25 SeitenA. KMC Introduction, Components & BenefitssantojuliansyahNoch keine Bewertungen
- Omni 1985 12 PDFDokument83 SeitenOmni 1985 12 PDFBrian GonzalezNoch keine Bewertungen
- What Is An Ibclc Flyer IlcaDokument2 SeitenWhat Is An Ibclc Flyer Ilcaapi-275110874Noch keine Bewertungen
- Gynae OncologyDokument52 SeitenGynae OncologyrkNoch keine Bewertungen
- U.S. Army Nurse Corps Fact SheetDokument7 SeitenU.S. Army Nurse Corps Fact SheetU.S. Army Medical Department (AMEDD)Noch keine Bewertungen
- Anestesia em Animais Silvestres Capitulo 1Dokument24 SeitenAnestesia em Animais Silvestres Capitulo 1Daniel CostaNoch keine Bewertungen
- WJMH 32 110Dokument6 SeitenWJMH 32 110Yacine Tarik AizelNoch keine Bewertungen
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (32)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (46)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (5)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (170)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisVon EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisBewertung: 5 von 5 Sternen5/5 (8)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)
- Troubled: A Memoir of Foster Care, Family, and Social ClassVon EverandTroubled: A Memoir of Foster Care, Family, and Social ClassBewertung: 4.5 von 5 Sternen4.5/5 (27)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingVon EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingBewertung: 4 von 5 Sternen4/5 (1138)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (254)