Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Management of Diabetic Foot Ulcers: A ReviewDokument8 SeitenManagement of Diabetic Foot Ulcers: A ReviewFitri Amelia RizkiNoch keine Bewertungen
- 02 Review On Artemisinine Derivatives For Malaria Control TANG Lin-HuaDokument38 Seiten02 Review On Artemisinine Derivatives For Malaria Control TANG Lin-HuaFitri Amelia RizkiNoch keine Bewertungen
- Antipsychotic Deprescribing Algorithm PDFDokument2 SeitenAntipsychotic Deprescribing Algorithm PDFFitri Amelia RizkiNoch keine Bewertungen
- ST T Classification Who ChapterDokument11 SeitenST T Classification Who ChapterFitri Amelia RizkiNoch keine Bewertungen
- Clinical and Experimental Advances in Congenital and Paediatric CataractsDokument16 SeitenClinical and Experimental Advances in Congenital and Paediatric CataractsFitri Amelia RizkiNoch keine Bewertungen
- 2015 Gout Classification CriteriaDokument12 Seiten2015 Gout Classification CriteriaVico RizkytaNoch keine Bewertungen
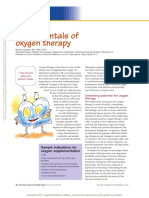
- Fundamentals of Oxygen Therapy.6Dokument3 SeitenFundamentals of Oxygen Therapy.6Fitri Amelia RizkiNoch keine Bewertungen
- Red Reflex Test: ProcedureDokument6 SeitenRed Reflex Test: ProcedureFitri Amelia RizkiNoch keine Bewertungen
- RefratDokument31 SeitenRefratFitri Amelia RizkiNoch keine Bewertungen
- Cataract: Care of The Adult Patient WithDokument43 SeitenCataract: Care of The Adult Patient WithAnna Francesca AbarquezNoch keine Bewertungen
- Infantile CataractDokument6 SeitenInfantile Cataractkartini ciatawiNoch keine Bewertungen
- Hyphema 2Dokument7 SeitenHyphema 2heidyNoch keine Bewertungen
- Ophthalmology Referral GuidelinesDokument9 SeitenOphthalmology Referral GuidelinesFitri Amelia RizkiNoch keine Bewertungen
- Glaucoma GuidelinesDokument28 SeitenGlaucoma GuidelinesRina RostianaNoch keine Bewertungen
- Ecr2015 c-1165Dokument28 SeitenEcr2015 c-1165Fitri Amelia RizkiNoch keine Bewertungen
- A Trevor's Disease HindawiDokument9 SeitenA Trevor's Disease HindawiFitri Amelia RizkiNoch keine Bewertungen
- Cios 4 107 PDFDokument10 SeitenCios 4 107 PDFFitri Amelia RizkiNoch keine Bewertungen
- THE Pathology OF Osteoclastoma OR Giant-Cell Tumour OF Bone: Willis, London, EnglandDokument5 SeitenTHE Pathology OF Osteoclastoma OR Giant-Cell Tumour OF Bone: Willis, London, EnglandFitri Amelia RizkiNoch keine Bewertungen
- Jurnal 2 - TBDokument8 SeitenJurnal 2 - TBFitri Amelia RizkiNoch keine Bewertungen
- Amniosentesis Dan CvsDokument13 SeitenAmniosentesis Dan CvsFitri Amelia RizkiNoch keine Bewertungen
- ABJS Volume 4 Issue 1 Pages 2-9Dokument8 SeitenABJS Volume 4 Issue 1 Pages 2-9Fitri Amelia RizkiNoch keine Bewertungen
- JurnalDokument4 SeitenJurnalFitri Amelia RizkiNoch keine Bewertungen
- EAU Extended Guidelines 2016 EdnDokument1.159 SeitenEAU Extended Guidelines 2016 Ednsamirmohd100% (1)
- Jurnal Konservatif ManagementDokument5 SeitenJurnal Konservatif ManagementFitri Amelia RizkiNoch keine Bewertungen
- Infection Control of Aerosol Transmissible DiseasesDokument53 SeitenInfection Control of Aerosol Transmissible DiseasesFitri Amelia RizkiNoch keine Bewertungen
- Emergency Medical Tech PPT Templates StandardDokument9 SeitenEmergency Medical Tech PPT Templates StandardFitri Amelia RizkiNoch keine Bewertungen
- Research Article: Outcome Predictors in First-Ever Ischemic Stroke Patients: A Population-Based StudyDokument9 SeitenResearch Article: Outcome Predictors in First-Ever Ischemic Stroke Patients: A Population-Based StudyFitri Amelia RizkiNoch keine Bewertungen
- Virtual Autopsy in Forensic Medicine-00085892Dokument4 SeitenVirtual Autopsy in Forensic Medicine-00085892Fitri Amelia RizkiNoch keine Bewertungen
- The Nervous System: Quicktime™ An D A Tiff (Uncompressed) Decompressor Are Need Ed To See This P IctureDokument26 SeitenThe Nervous System: Quicktime™ An D A Tiff (Uncompressed) Decompressor Are Need Ed To See This P IcturecamixxxNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 6 0LDies PDFDokument101 Seiten6 0LDies PDFscodavnx100% (1)
- Surgical Sutures: Suture SizeDokument7 SeitenSurgical Sutures: Suture SizeMei PayumoNoch keine Bewertungen
- Modeling COVID-19 Epidemics in An Excel SpreadsheeDokument15 SeitenModeling COVID-19 Epidemics in An Excel SpreadsheeMagesha kumarNoch keine Bewertungen
- Principles of Communication Reviewer MidtermDokument5 SeitenPrinciples of Communication Reviewer MidtermVon Ryan AlcazarNoch keine Bewertungen
- TacheometryDokument6 SeitenTacheometryregieNoch keine Bewertungen
- 1520 0477 Bams D 22 0164.1Dokument22 Seiten1520 0477 Bams D 22 0164.1Slobodna DalmacijaNoch keine Bewertungen
- Maths - 2B Imp QuestionsDokument93 SeitenMaths - 2B Imp QuestionsBandaru Chiranjeevi100% (1)
- Inorganic Chemistry 2 Main Exam (3) and MemoDokument11 SeitenInorganic Chemistry 2 Main Exam (3) and MemoKgasu MosaNoch keine Bewertungen
- 88543-Activity Week 3 (Language of Mathematics)Dokument2 Seiten88543-Activity Week 3 (Language of Mathematics)Mylene L RimandoNoch keine Bewertungen
- 9.coordination CompoundsDokument46 Seiten9.coordination CompoundsSeenu MNoch keine Bewertungen
- Programming Exercise 2Dokument2 SeitenProgramming Exercise 2hamidahrazakNoch keine Bewertungen
- On The Coupling of Mechanics With Bioelectricity and Its Role in MorphogenesisDokument12 SeitenOn The Coupling of Mechanics With Bioelectricity and Its Role in MorphogenesisVishvendraNoch keine Bewertungen
- Tutorial Summary: 3D Example: Magneto Thermal ApplicationDokument3 SeitenTutorial Summary: 3D Example: Magneto Thermal ApplicationAndrewNoch keine Bewertungen
- Mongo DB Basic CommandsDokument15 SeitenMongo DB Basic CommandsgauriNoch keine Bewertungen
- U Center UserGuide (UBX 13005250)Dokument94 SeitenU Center UserGuide (UBX 13005250)Phi Ra Uch100% (1)
- 3Dokument8 Seiten3K@mR@N D@uD P@nHw@RNoch keine Bewertungen
- Price DeterminationDokument2 SeitenPrice DeterminationSikander BehalNoch keine Bewertungen
- Chapter 5Dokument23 SeitenChapter 5Anil RaiNoch keine Bewertungen
- AndroidDokument61 SeitenAndroidNamithaNoch keine Bewertungen
- Audi A6 2.7t Component LocationDokument3 SeitenAudi A6 2.7t Component LocationLucian MicurescuNoch keine Bewertungen
- Penlon-Paragon AV-S-Ventilator - User ManualDokument72 SeitenPenlon-Paragon AV-S-Ventilator - User Manualrkillian44Noch keine Bewertungen
- Gajendra Singh (ONGC Training Report)Dokument55 SeitenGajendra Singh (ONGC Training Report)Gajju12567% (6)
- Conversion & Reactor Sizing: Dr. Kelly Yong Tau LenDokument16 SeitenConversion & Reactor Sizing: Dr. Kelly Yong Tau LenAmandaEdwinNoch keine Bewertungen
- 1-B SC (Maths)Dokument22 Seiten1-B SC (Maths)Prashant GuptaNoch keine Bewertungen
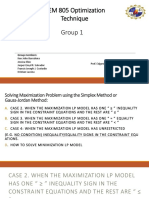
- Optimization Technique Group 1Dokument60 SeitenOptimization Technique Group 1jmlafortezaNoch keine Bewertungen
- A Simple Favor 2018 720p BluRay x264 - (YTS AM) mp4Dokument2 SeitenA Simple Favor 2018 720p BluRay x264 - (YTS AM) mp4Dewi SartikaNoch keine Bewertungen
- GOC & EAS CPP-II - PMDDokument14 SeitenGOC & EAS CPP-II - PMDVansh sareenNoch keine Bewertungen
- GusekDokument177 SeitenGusekAitorAlbertoBaezNoch keine Bewertungen
- Piezoelectric Generator Harvesting Bike VibrationsDokument7 SeitenPiezoelectric Generator Harvesting Bike VibrationsVladimir VladimirNoch keine Bewertungen
- APN-002 Protection and Control DevicesDokument10 SeitenAPN-002 Protection and Control DevicesYusron MuhammadNoch keine Bewertungen