Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Nonbinary HormonesDokument9 SeitenNonbinary HormonesBiniam GrafféNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Clinical Research Overview DownloadDokument13 SeitenClinical Research Overview DownloadWILLIAM RICARDO CASTAÑEDA VARGASNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Global Submission On IndDokument16 SeitenGlobal Submission On IndRahul PalsNoch keine Bewertungen
- Grastric Gavage & LavageDokument17 SeitenGrastric Gavage & LavageJuliet Pua74% (19)
- DERMAPENDokument33 SeitenDERMAPENAriadna Roca100% (6)
- Pharmacology of SulfonamidesDokument37 SeitenPharmacology of SulfonamidesDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Neurology revision-2015: Benztropine side effects & status epilepticus treatmentsDokument99 SeitenNeurology revision-2015: Benztropine side effects & status epilepticus treatmentsPaz Vida100% (7)
- 6 BDokument2 Seiten6 BZafar KhanNoch keine Bewertungen
- Aqa Bya3 W QP Jan08Dokument16 SeitenAqa Bya3 W QP Jan08Zafar KhanNoch keine Bewertungen
- UntitledDokument1 SeiteUntitledZafar KhanNoch keine Bewertungen
- General Certificate of Education January 2008 Advanced Subsidiary ExaminationDokument20 SeitenGeneral Certificate of Education January 2008 Advanced Subsidiary ExaminationZafar KhanNoch keine Bewertungen
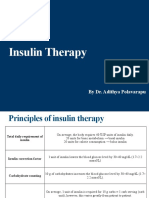
- Insulin Therapy: by Dr. Adithya PolavarapuDokument18 SeitenInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNoch keine Bewertungen
- Drugs That May Unmask or Worsen Myasthenia GravisDokument2 SeitenDrugs That May Unmask or Worsen Myasthenia GravisnuriajiNoch keine Bewertungen
- BMH-NM Surgical Site Infection Reduction Poster 04162021Dokument1 SeiteBMH-NM Surgical Site Infection Reduction Poster 04162021Baptist Memorial Health CareNoch keine Bewertungen
- Unit 08 Client Assessment Matrix Carl Fitt ProsDokument2 SeitenUnit 08 Client Assessment Matrix Carl Fitt Prosapi-312576381Noch keine Bewertungen
- 1 Lines EsofagoDokument33 Seiten1 Lines EsofagoClaudia MartínezNoch keine Bewertungen
- No. Kode Nama Obat /barang Stok Komputer Stok Sistem SelisihDokument39 SeitenNo. Kode Nama Obat /barang Stok Komputer Stok Sistem SelisihniluhandyaNoch keine Bewertungen
- BIOAVAILABILITY KEY FACTSDokument38 SeitenBIOAVAILABILITY KEY FACTSsaadNoch keine Bewertungen
- L 2 Terminology of DrugsDokument29 SeitenL 2 Terminology of DrugsVianesa RiberuNoch keine Bewertungen
- KetorolacDokument16 SeitenKetorolacniken retnoNoch keine Bewertungen
- TramadolDokument3 SeitenTramadolMark Joseph Mabazza LappayNoch keine Bewertungen
- workshop-PV TrainingDokument36 Seitenworkshop-PV TrainingHala MohamedNoch keine Bewertungen
- PhytosomesDokument3 SeitenPhytosomesSingh TaminderjitNoch keine Bewertungen
- Top 200 Drugs in OrderDokument7 SeitenTop 200 Drugs in OrderEamon BarkhordarianNoch keine Bewertungen
- Drugs Used For Conscious SedationDokument1 SeiteDrugs Used For Conscious SedationonslowmoNoch keine Bewertungen
- Maintenance Plan & Restorative Phase Guidelines For IMPLANTDokument5 SeitenMaintenance Plan & Restorative Phase Guidelines For IMPLANTPaylip Dental LaboratoryNoch keine Bewertungen
- Repro Quiz 3 NishantDokument2 SeitenRepro Quiz 3 NishantNishantNoch keine Bewertungen
- Code Registration Number Strength Presentation Form AgentDokument30 SeitenCode Registration Number Strength Presentation Form AgentA GhNoch keine Bewertungen
- Dose Adjustment in Patients With Liver DiseaseDokument17 SeitenDose Adjustment in Patients With Liver DiseaseNurul Fitrializa ElfNoch keine Bewertungen
- VRD Bortezomib Lenalidomide Dexamethasone Multiple Myeloma Protocol V1.0Dokument9 SeitenVRD Bortezomib Lenalidomide Dexamethasone Multiple Myeloma Protocol V1.0gini erwantiNoch keine Bewertungen
- Cefaleia - ContinuumDokument195 SeitenCefaleia - ContinuumRafaelNoch keine Bewertungen
- Pharmaceuticals For Small Animal Internal Medicine PreparationDokument11 SeitenPharmaceuticals For Small Animal Internal Medicine Preparationahmet öztürkNoch keine Bewertungen
- DrugBank - Erythromycin (DB00199)Dokument18 SeitenDrugBank - Erythromycin (DB00199)Nuril FahmiNoch keine Bewertungen