Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Pregnancy Following Miscarriage What Is The Optimum Interpregnancy IntervalDokument3 SeitenPregnancy Following Miscarriage What Is The Optimum Interpregnancy IntervallcmurilloNoch keine Bewertungen
- Everyday Contraception ConsiderationsDokument15 SeitenEveryday Contraception ConsiderationslcmurilloNoch keine Bewertungen
- Obgm Feb2018 Vol.30 No.2 PDFDokument55 SeitenObgm Feb2018 Vol.30 No.2 PDFlcmurilloNoch keine Bewertungen
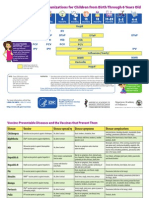
- Parent Ver SCH 0 6yrsDokument2 SeitenParent Ver SCH 0 6yrslcmurilloNoch keine Bewertungen
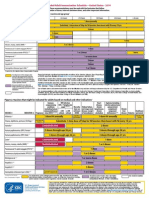
- Catchup Schedule BWDokument4 SeitenCatchup Schedule BWlcmurilloNoch keine Bewertungen
- Adult ScheduleDokument3 SeitenAdult SchedulelcmurilloNoch keine Bewertungen
- Adult Schedule 11x17Dokument2 SeitenAdult Schedule 11x17lcmurilloNoch keine Bewertungen
- Adult Combined ScheduleDokument5 SeitenAdult Combined SchedulelcmurilloNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- PE 10 3rd QuarterDokument20 SeitenPE 10 3rd QuarterIrish Lea May Pacamalan100% (2)
- Stanhouse C. Ivy v. Elizabeth H. Dole, Secretary of Transportation, 811 F.2d 1505, 4th Cir. (1987)Dokument3 SeitenStanhouse C. Ivy v. Elizabeth H. Dole, Secretary of Transportation, 811 F.2d 1505, 4th Cir. (1987)Scribd Government DocsNoch keine Bewertungen
- Constitutional Law NotesDokument38 SeitenConstitutional Law NotesMarius Damian100% (1)
- Gonzales vs. Judge BersaminDokument3 SeitenGonzales vs. Judge BersaminJp Karl Gonzales UliganNoch keine Bewertungen
- Bullying Research PaperDokument11 SeitenBullying Research Paperapi-528889036Noch keine Bewertungen
- First Information ReportDokument4 SeitenFirst Information ReportYedavelli BadrinathNoch keine Bewertungen
- 2015 2023 PDFDokument22 Seiten2015 2023 PDFBinibining KoreaNoch keine Bewertungen
- 45 Important Question On The Magadha EmpireDokument4 Seiten45 Important Question On The Magadha Empirevenkatv1986Noch keine Bewertungen
- Pope Francis Tells YOUNG PEOPLEDokument4 SeitenPope Francis Tells YOUNG PEOPLEJoseph VincentNoch keine Bewertungen
- 6 Velasquez, Jr. V Lisondra LandDokument2 Seiten6 Velasquez, Jr. V Lisondra LandAngelica Bautista100% (1)
- People vs. Royol - G.R. No. 224297 - February 13, 2019 - Criminal LawDokument2 SeitenPeople vs. Royol - G.R. No. 224297 - February 13, 2019 - Criminal LawAndres SoguilonNoch keine Bewertungen
- 06 AbbreviationDokument3 Seiten06 AbbreviationAkash VermaNoch keine Bewertungen
- Land Titles and Deeds: Paulito M. Punongbayan Llb2ADokument27 SeitenLand Titles and Deeds: Paulito M. Punongbayan Llb2Apaul2574Noch keine Bewertungen
- Just The Way You AreDokument2 SeitenJust The Way You AreMA. BRIELLE CASSIDY SOLPICONoch keine Bewertungen
- DigestDokument3 SeitenDigestgalileo roma iiiNoch keine Bewertungen
- Dhan Guru Nanak - PresentationDokument19 SeitenDhan Guru Nanak - PresentationTaranveer Singh100% (1)
- Insanity PleaDokument8 SeitenInsanity Pleaapi-545890787Noch keine Bewertungen
- Presentazione ArielDokument20 SeitenPresentazione ArielAngel De OliveiraNoch keine Bewertungen
- 2010 Kansas Department of Wildlife and Parks Fall Hunting AtlasDokument76 Seiten2010 Kansas Department of Wildlife and Parks Fall Hunting AtlasRoeHuntingNoch keine Bewertungen
- Hilongos, LeyteDokument2 SeitenHilongos, LeyteSunStar Philippine NewsNoch keine Bewertungen
- Vessel HandlingDokument64 SeitenVessel Handlingderantague100% (1)
- Times Leader 05-31-2013Dokument38 SeitenTimes Leader 05-31-2013The Times LeaderNoch keine Bewertungen
- Spouses Anchevara and Valdez V Ramos G.R. No. 175172, September 29, 2009Dokument12 SeitenSpouses Anchevara and Valdez V Ramos G.R. No. 175172, September 29, 2009ChatNoch keine Bewertungen
- Memories of Childhood's Slavery Days by Burton, Annie L., 1858Dokument41 SeitenMemories of Childhood's Slavery Days by Burton, Annie L., 1858Gutenberg.orgNoch keine Bewertungen
- Fighting Serbs, Mihailovich and Yugoslavia Ruth MitchellDokument34 SeitenFighting Serbs, Mihailovich and Yugoslavia Ruth MitchellAleksandar Stosich50% (2)
- RTK 7777-R State Road (Public Property)Dokument18 SeitenRTK 7777-R State Road (Public Property)christoofar2190Noch keine Bewertungen
- The Thief's StoryDokument7 SeitenThe Thief's Storyrakeshkmr411Noch keine Bewertungen
- Petitioner Vs Vs Respondent: Second DivisionDokument12 SeitenPetitioner Vs Vs Respondent: Second DivisionSeonoNoch keine Bewertungen
- Goya Foods, Inc. v. Unanue, 290 F.3d 63, 1st Cir. (2002)Dokument20 SeitenGoya Foods, Inc. v. Unanue, 290 F.3d 63, 1st Cir. (2002)Scribd Government DocsNoch keine Bewertungen
- Catalog 2012 RossiDokument19 SeitenCatalog 2012 Rossitublin601Noch keine Bewertungen