Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Somalia's Federal Parliament Elects Speakers, Deputy SpeakersDokument3 SeitenSomalia's Federal Parliament Elects Speakers, Deputy SpeakersAMISOM Public Information ServicesNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Letter To The FTB of California Regarding The Lies and Deceit Purveyed by Micheal Hamersley of Hamersley Partneres The Lying Murdering Faux Tax Shelter CrusaderDokument5 SeitenLetter To The FTB of California Regarding The Lies and Deceit Purveyed by Micheal Hamersley of Hamersley Partneres The Lying Murdering Faux Tax Shelter Crusaderkpmgtaxshelter_kpmg tax shelter-kpmg tax shelterNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- PLSQL Cig1Dokument2 SeitenPLSQL Cig1ram5584Noch keine Bewertungen
- Parliament's SovereigntyDokument2 SeitenParliament's SovereigntyFatimah Jŭiĉes ChaiNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Public Officer - Avenido Vs CSCDokument5 SeitenPublic Officer - Avenido Vs CSCMaria Linda GabitNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- RIZALDokument6 SeitenRIZALZeny Ann MolinaNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- GBMLT V Malinao - Arcellana (2017)Dokument2 SeitenGBMLT V Malinao - Arcellana (2017)Patrick Violago ArcellanaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Maine ConstitutionDokument37 SeitenMaine Constitutionthisdog100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Proverbs 31:1-3 (KJV) : 1 The Words of King Lemuel, The Prophecy That His Mother Taught HimDokument12 SeitenProverbs 31:1-3 (KJV) : 1 The Words of King Lemuel, The Prophecy That His Mother Taught HimMaradine TepNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Thirteen Colonies - ConnecticutDokument145 SeitenThe Thirteen Colonies - Connecticutsperry100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Home Invasion: Robbers Disclose What You Should KnowDokument19 SeitenHome Invasion: Robbers Disclose What You Should KnowLittleWhiteBakkie100% (2)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Structure & Function of Erototoxic-Pornographic Sexual MediaDokument1 SeiteThe Structure & Function of Erototoxic-Pornographic Sexual MediaJudith Reisman, Ph.D.Noch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- EMT 9/11 Memorial Letter To The EditorDokument2 SeitenEMT 9/11 Memorial Letter To The EditorZachary WestNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- SK Internal Rules of Procedures, SkchairgpadiatonDokument12 SeitenSK Internal Rules of Procedures, SkchairgpadiatonGp Marshall Adiaton75% (4)
- The True, Real, and Public Woman Portrayed in Ruth HallDokument16 SeitenThe True, Real, and Public Woman Portrayed in Ruth HallElizabethNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- United States v. Femia, 1st Cir. (1995)Dokument52 SeitenUnited States v. Femia, 1st Cir. (1995)Scribd Government DocsNoch keine Bewertungen
- People v. Umali - Full TextDokument6 SeitenPeople v. Umali - Full TextjiggerNoch keine Bewertungen
- Fallen Angel Chapter OneDokument19 SeitenFallen Angel Chapter OneDez Donaire100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- From Mulla Ali Qari's AsrarDokument1 SeiteFrom Mulla Ali Qari's AsrarAsma HussainNoch keine Bewertungen
- People Vs Arnulfo FernandezDokument1 SeitePeople Vs Arnulfo FernandezCharles Roger Raya100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Lajave vs. Javellana DigestDokument4 SeitenLajave vs. Javellana DigestEmir Mendoza100% (3)
- Charles Walker. Reflections of Tupac AmaruDokument4 SeitenCharles Walker. Reflections of Tupac AmaruHenry TantaleánNoch keine Bewertungen
- Atty Agubamemorandum of AgreementDokument2 SeitenAtty Agubamemorandum of AgreementBayan Ng RamonNoch keine Bewertungen
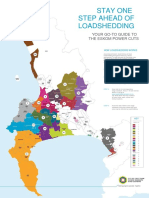
- Load Shedding All Areas Schedule and MapDokument2 SeitenLoad Shedding All Areas Schedule and MapRobin VisserNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Memo Re NakayamaDokument2 SeitenMemo Re NakayamaLatoya StewartNoch keine Bewertungen
- V For Vendetta EssayDokument5 SeitenV For Vendetta Essayapi-302433885Noch keine Bewertungen
- Report of The 7th ANMCC, 2021Dokument14 SeitenReport of The 7th ANMCC, 2021A AASHIK KAREEM nalsarNoch keine Bewertungen
- 0 Test PredictivviithDokument3 Seiten0 Test PredictivviithmirabikaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Petitioners, vs. HEIRS OF ROBERTO CUTANDA, Namely, GERVACIO CUTANDADokument7 SeitenPetitioners, vs. HEIRS OF ROBERTO CUTANDA, Namely, GERVACIO CUTANDAayleenNoch keine Bewertungen
- Politicka Misao 1 2011 94 107 PDFDokument14 SeitenPoliticka Misao 1 2011 94 107 PDFmilan trifunovicNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)