Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Pengganti DecolgenDokument2 SeitenPengganti DecolgenVeysusanNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Pengganti DecolgenDokument2 SeitenPengganti DecolgenVeysusanNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- DAPUS (Kurang Pny Edwin)Dokument1 SeiteDAPUS (Kurang Pny Edwin)VeysusanNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Cerebrovascular Disease, 1-62: Dapus PTO 2Dokument1 SeiteCerebrovascular Disease, 1-62: Dapus PTO 2VeysusanNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Prepare and Mix Syrups For Food or Related Product ProductionDokument4 SeitenPrepare and Mix Syrups For Food or Related Product ProductionVeysusanNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Interview (3 Minutes) : (The Students Hand Their Mark Sheets To The Examiner)Dokument8 SeitenInterview (3 Minutes) : (The Students Hand Their Mark Sheets To The Examiner)VeysusanNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grafik Persamaan Kurva Baku Absorbansi Vs KonsentrasiDokument2 SeitenGrafik Persamaan Kurva Baku Absorbansi Vs KonsentrasiVeysusanNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Print Kurva Lap StabiloDokument5 SeitenPrint Kurva Lap StabiloVeysusanNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Protokol KemoDokument13 SeitenProtokol KemoVeysusanNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Primary CharactersticsDokument5 SeitenPrimary CharactersticsVeysusanNoch keine Bewertungen
- We Are The B / B Class LifeDokument3 SeitenWe Are The B / B Class LifeVeysusanNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- RCT Appraisal Sheets 2005 English-2Dokument3 SeitenRCT Appraisal Sheets 2005 English-2VeysusanNoch keine Bewertungen
- Buku Panduan Kepengurusan KMBK Dharma Virya 2011 / 2012Dokument1 SeiteBuku Panduan Kepengurusan KMBK Dharma Virya 2011 / 2012VeysusanNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Laporan Pertanggungjawaban Malam Keakraban (Makrab) : "Together in Different"Dokument1 SeiteLaporan Pertanggungjawaban Malam Keakraban (Makrab) : "Together in Different"VeysusanNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Data Pengamatan 1Dokument13 SeitenData Pengamatan 1VeysusanNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- What Makes U BeautifulDokument1 SeiteWhat Makes U BeautifulVeysusanNoch keine Bewertungen
- R M - Paulus Bambang Irawan, SJ Sr. M. Theresia Farjanti H. RGSDokument2 SeitenR M - Paulus Bambang Irawan, SJ Sr. M. Theresia Farjanti H. RGSVeysusanNoch keine Bewertungen
- Cover Proposal Makrab 2013Dokument1 SeiteCover Proposal Makrab 2013VeysusanNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- 2bic & Davichi - A Night Like This LyricsDokument2 Seiten2bic & Davichi - A Night Like This LyricsVeysusanNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Wo Men Yi Qi Chi Laomu de Fan, He Laomu de Shui, Xi Tong Yang de Kong QiDokument2 SeitenWo Men Yi Qi Chi Laomu de Fan, He Laomu de Shui, Xi Tong Yang de Kong QiVeysusanNoch keine Bewertungen
- Tactical Radio BasicsDokument46 SeitenTactical Radio BasicsJeff Brissette100% (2)
- Canon IR2016J Error Code ListDokument4 SeitenCanon IR2016J Error Code ListZahidShaikhNoch keine Bewertungen
- PDF Applied Failure Analysis 1 NSW - CompressDokument2 SeitenPDF Applied Failure Analysis 1 NSW - CompressAgungNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- CHAPTER 22-Audit Evidence EvaluationDokument27 SeitenCHAPTER 22-Audit Evidence EvaluationIryne Kim PalatanNoch keine Bewertungen
- UN - Towards Sustainable DevelopmentDokument17 SeitenUN - Towards Sustainable Developmentviva_33Noch keine Bewertungen
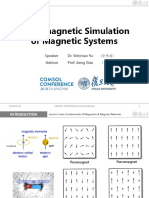
- Micromagnetic Simulation of Magnetic SystemsDokument12 SeitenMicromagnetic Simulation of Magnetic SystemsImri SsNoch keine Bewertungen
- EAU 2022 - Prostate CancerDokument229 SeitenEAU 2022 - Prostate Cancerpablo penguinNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Unit 4 Pharmacognsosy 2 - 5th SemDokument16 SeitenUnit 4 Pharmacognsosy 2 - 5th SemJagadeeshkeerthi KeerthiNoch keine Bewertungen
- Media DRIVEON Vol25 No2Dokument21 SeitenMedia DRIVEON Vol25 No2Nagenthara PoobathyNoch keine Bewertungen
- Daftar Kalibrasi Peralatan MedisDokument34 SeitenDaftar Kalibrasi Peralatan Medisdiklat rssnNoch keine Bewertungen
- Activity Diagram 1Dokument14 SeitenActivity Diagram 1Yousef GamalNoch keine Bewertungen
- Notice: Customhouse Broker License Cancellation, Suspension, Etc.Dokument2 SeitenNotice: Customhouse Broker License Cancellation, Suspension, Etc.Justia.comNoch keine Bewertungen
- Precision Probability Index (Elf)Dokument20 SeitenPrecision Probability Index (Elf)EdsonnSPBrNoch keine Bewertungen
- Power of Company Law BoardDokument21 SeitenPower of Company Law Boardraman raghavNoch keine Bewertungen
- An Introduction To SAP Business One CloudDokument14 SeitenAn Introduction To SAP Business One CloudBharathkumar PalaniveluNoch keine Bewertungen
- How To Apply For The UpcatDokument3 SeitenHow To Apply For The UpcatAaron ReyesNoch keine Bewertungen
- GG&G 2012 CatDokument111 SeitenGG&G 2012 Cattyrant88Noch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Mortal Kombat XDokument24 SeitenMortal Kombat XMindSpaceApocalypseNoch keine Bewertungen
- Orphanage Project ProposalDokument3 SeitenOrphanage Project ProposaldtimtimanNoch keine Bewertungen
- Excel Tips TricksDokument26 SeitenExcel Tips Tricksskondra12Noch keine Bewertungen
- Essays From Previous Years For HseeDokument2 SeitenEssays From Previous Years For HseeGagan TottempudiNoch keine Bewertungen
- Leadership Assesment ToolDokument5 SeitenLeadership Assesment ToolJayeeta DebnathNoch keine Bewertungen
- Book of Abstracts: Philippine Projects To The Intel International Science and Engineering FairDokument84 SeitenBook of Abstracts: Philippine Projects To The Intel International Science and Engineering FairJimarie BithaoNoch keine Bewertungen
- LTE Radio Network Design Guideline (FDD)Dokument33 SeitenLTE Radio Network Design Guideline (FDD)Tri Frida NingrumNoch keine Bewertungen
- Pas 38 Pas 41 Pas 40Dokument12 SeitenPas 38 Pas 41 Pas 40Leddie Bergs Villanueva VelascoNoch keine Bewertungen
- RODEL LUZ y ONG, Petitioner, People of The Philippines, Respondent. FactsDokument1 SeiteRODEL LUZ y ONG, Petitioner, People of The Philippines, Respondent. FactsBee Raagas100% (1)
- Ten Rules of NetiquetteDokument11 SeitenTen Rules of NetiquetteAriel CancinoNoch keine Bewertungen
- The US Navy - Fact File - MQ-8C Fire ScoutDokument2 SeitenThe US Navy - Fact File - MQ-8C Fire ScoutAleksei KarpaevNoch keine Bewertungen
- Bitmicro Case Complainants PositionDokument19 SeitenBitmicro Case Complainants PositionNoy SorianoNoch keine Bewertungen
- Bonus 6 - Mastering ASP - NET Core SecurityDokument147 SeitenBonus 6 - Mastering ASP - NET Core SecurityDark Shadow100% (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (32)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)