Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Curtis - Ramsden (2016) Emergency and Trauma Care For Nurses and ParamedicsDokument1.406 SeitenCurtis - Ramsden (2016) Emergency and Trauma Care For Nurses and ParamedicsSangid Yahya100% (5)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hypnosis Principles and Applications. An Adjunct To Anesthesia - M.R. EslingerDokument8 SeitenHypnosis Principles and Applications. An Adjunct To Anesthesia - M.R. EslingerNiky GiaccioNoch keine Bewertungen
- SL 4 Test Questions GeneticsDokument16 SeitenSL 4 Test Questions GeneticsAllison Khoo100% (1)
- Williams ObstetricsDokument2 SeitenWilliams Obstetricsmely sandyNoch keine Bewertungen
- Sleep Disorder Classification-AASMDokument208 SeitenSleep Disorder Classification-AASMJoy100% (2)
- Alsa Excell 400 - User Manual PDFDokument30 SeitenAlsa Excell 400 - User Manual PDFSamoel De MeloNoch keine Bewertungen
- This Is Lean BookDokument90 SeitenThis Is Lean BookGabriel C JoseNoch keine Bewertungen
- Trends in Development of Nursing Education in IndiaDokument22 SeitenTrends in Development of Nursing Education in IndiaShyam82% (11)
- Daradia Pain Hospital, The Exclusive Pain Management Hospital, Not Only Treats Pain, But Also Organizes Pain Management Courses To Train PhysiciansDokument2 SeitenDaradia Pain Hospital, The Exclusive Pain Management Hospital, Not Only Treats Pain, But Also Organizes Pain Management Courses To Train PhysiciansPR.comNoch keine Bewertungen
- 1 Whostomachchapter3Dokument1 Seite1 Whostomachchapter3Gabriela MilitaruNoch keine Bewertungen
- Resume Manoj R.kandoiDokument9 SeitenResume Manoj R.kandoiManoj KandoiNoch keine Bewertungen
- Radiology Fellowships - Austin HealthDokument4 SeitenRadiology Fellowships - Austin Healthsage masonNoch keine Bewertungen
- Reviewer: Mendelian Inheritance X-Linked Dominant Inheritance X-Linked Dominant InheritanceDokument3 SeitenReviewer: Mendelian Inheritance X-Linked Dominant Inheritance X-Linked Dominant InheritanceMary Rose FabianNoch keine Bewertungen
- DR SivaSubrmaniamDokument4 SeitenDR SivaSubrmaniamAyya R.vishwanathan MuthariyarNoch keine Bewertungen
- QCIDokument27 SeitenQCIerpNoch keine Bewertungen
- Infection, Genetics and Evolution: Ahmed Ahmed, Richard M. Anthony, Rudy A. HartskeerlDokument8 SeitenInfection, Genetics and Evolution: Ahmed Ahmed, Richard M. Anthony, Rudy A. Hartskeerlvignesh9489Noch keine Bewertungen
- ACOG JournalDokument7 SeitenACOG JournalMarvin OcampoNoch keine Bewertungen
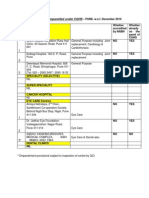
- CGHS Hosp Pune ListDokument4 SeitenCGHS Hosp Pune Listmak_iofsNoch keine Bewertungen
- Uva 20cover 20letterDokument1 SeiteUva 20cover 20letterapi-302868411Noch keine Bewertungen
- Government of Andhra Pradesh AbsractDokument9 SeitenGovernment of Andhra Pradesh Absract2588001Noch keine Bewertungen
- PartogramDokument3 SeitenPartogrammuchalaithNoch keine Bewertungen
- 2019 Pre-Enrolment Physical - Medical Examination Guidelines For UPLB FreshmanDokument1 Seite2019 Pre-Enrolment Physical - Medical Examination Guidelines For UPLB FreshmanAnna Izabelle SeyerNoch keine Bewertungen
- HSMT 2101 Group PaperDokument7 SeitenHSMT 2101 Group Paperapi-490176265Noch keine Bewertungen
- Example Multiple-Choice Questions (MCQS) : Only One Answer Is Correct - It Can Be Found at The BottomDokument2 SeitenExample Multiple-Choice Questions (MCQS) : Only One Answer Is Correct - It Can Be Found at The BottomDrSheika Bawazir0% (1)
- IUGA Scoring SystemDokument40 SeitenIUGA Scoring SystemBudi Iman SantosoNoch keine Bewertungen
- TrikoepiteliomaDokument39 SeitenTrikoepiteliomaNovy TriandaniNoch keine Bewertungen
- Pediatrics 2002 Ballard E63Dokument8 SeitenPediatrics 2002 Ballard E63dentistalitNoch keine Bewertungen
- Human IdentificationDokument5 SeitenHuman IdentificationdianjabalNoch keine Bewertungen
- Red Reflex Examination in Neonates, Infants, and Children: Policy StatementDokument7 SeitenRed Reflex Examination in Neonates, Infants, and Children: Policy StatementMilly Carcelén JiménezNoch keine Bewertungen
- Certificate IV in PathologyDokument6 SeitenCertificate IV in PathologyUpul EdirisingheNoch keine Bewertungen