Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Young Schema QuestionnaireDokument8 SeitenYoung Schema QuestionnaireDaiana Da100% (5)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Random FactsDokument353 SeitenRandom FactsSergio Rivas100% (1)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- HIPULSE U 80kVA 500kVA-Manual - V1.1Dokument157 SeitenHIPULSE U 80kVA 500kVA-Manual - V1.1joseph mendezNoch keine Bewertungen
- Linkage 2 Lab ReportDokument25 SeitenLinkage 2 Lab Reportapi-25176084883% (6)
- Educatia Prin Iubire Ross Campbell1Dokument124 SeitenEducatia Prin Iubire Ross Campbell1harsandNoch keine Bewertungen
- Educatia Prin Iubire Ross Campbell1Dokument124 SeitenEducatia Prin Iubire Ross Campbell1harsandNoch keine Bewertungen
- Black White Women CancerDokument24 SeitenBlack White Women CancerDaiana DaNoch keine Bewertungen
- Breast Cancer CopingDokument9 SeitenBreast Cancer CopingDaiana DaNoch keine Bewertungen
- Articulo de Las 3 Tesis Por BrowDokument30 SeitenArticulo de Las 3 Tesis Por BrowJHIMI DEIVIS QUISPE ROQUENoch keine Bewertungen
- Nfpa Training - Nfpa 72Dokument107 SeitenNfpa Training - Nfpa 72yusuf.ahmediutNoch keine Bewertungen
- Naming Alcohols, Aldehydes. EtcDokument1 SeiteNaming Alcohols, Aldehydes. Etcim_mikezNoch keine Bewertungen
- 9701 w03 QP 4Dokument12 Seiten9701 w03 QP 4Hubbak KhanNoch keine Bewertungen
- PED16 Foundation of Inclusive Special EducationDokument56 SeitenPED16 Foundation of Inclusive Special EducationCHARESS MARSAMOLO TIZONNoch keine Bewertungen
- Adjectives Comparative and Superlative FormDokument5 SeitenAdjectives Comparative and Superlative FormOrlando MiguelNoch keine Bewertungen
- Gastroschisis and Omphalocele PDFDokument8 SeitenGastroschisis and Omphalocele PDFUtama puteraNoch keine Bewertungen
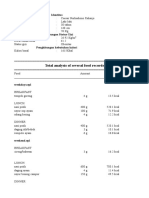
- Tugas Gizi Caesar Nurhadiono RDokument2 SeitenTugas Gizi Caesar Nurhadiono RCaesar 'nche' NurhadionoNoch keine Bewertungen
- Pengaruh Pembangunan Center Point of IndDokument11 SeitenPengaruh Pembangunan Center Point of IndSumitro SafiuddinNoch keine Bewertungen
- 742210V01Dokument2 Seiten742210V01hakim_zadehNoch keine Bewertungen
- EarthWear Clothier MaterialsDokument1 SeiteEarthWear Clothier MaterialsZhining LimNoch keine Bewertungen
- Operator's Manual: SE Series Slab ScissorsDokument52 SeitenOperator's Manual: SE Series Slab ScissorsthuanNoch keine Bewertungen
- Potential Prospect 1.7Dokument6 SeitenPotential Prospect 1.7Joshua M. GenoviaNoch keine Bewertungen
- Campus DrinkingDokument2 SeitenCampus DrinkingLiHertzi DesignNoch keine Bewertungen
- Dryden, 1994Dokument17 SeitenDryden, 1994Merve KurunNoch keine Bewertungen
- 01 Mono Channel BurnerDokument1 Seite01 Mono Channel BurnerSelwyn MunatsiNoch keine Bewertungen
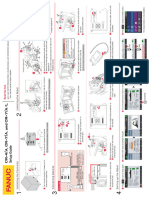
- CR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)Dokument1 SeiteCR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)lidiia.pavlkukNoch keine Bewertungen
- SCI Fayette Greene..2007-2009 ViolationsDokument10 SeitenSCI Fayette Greene..2007-2009 ViolationsHRCFedUpNoch keine Bewertungen
- Anesthesia 3Dokument24 SeitenAnesthesia 3PM Basiloy - AloNoch keine Bewertungen
- Io (Jupiter Moon)Dokument2 SeitenIo (Jupiter Moon)FatimaNoch keine Bewertungen
- Audio AmplifierDokument8 SeitenAudio AmplifierYuda Aditama100% (2)
- Lesson 1 Animal CareDokument8 SeitenLesson 1 Animal CareLexi PetersonNoch keine Bewertungen
- Datasheet Cofraplus 60Dokument2 SeitenDatasheet Cofraplus 60Žarko JanjićNoch keine Bewertungen
- Uji Stabilitas Tablet Floating Ranitidin HCL: Pengaruhnya Terhadap Sifat Fisik Dan Profil Disolusi Dalam Medium SGF Tanpa PepsinDokument16 SeitenUji Stabilitas Tablet Floating Ranitidin HCL: Pengaruhnya Terhadap Sifat Fisik Dan Profil Disolusi Dalam Medium SGF Tanpa PepsinZeaa MaysNoch keine Bewertungen
- Lab Safety RulesDokument2 SeitenLab Safety RulesChristine ManuelNoch keine Bewertungen
- 8582d Soldering Station English User GuideDokument9 Seiten8582d Soldering Station English User Guide1valdasNoch keine Bewertungen
- Industrial Attachment ReportDokument34 SeitenIndustrial Attachment ReportOtsile Charisma Otsile Saq100% (1)