Das könnte Ihnen auch gefallen
- Mhealth Business in NigeriaDokument23 SeitenMhealth Business in NigeriaAdesina IluyemiNoch keine Bewertungen
- Wireless Healthcare Asset Management Second EditionVon EverandWireless Healthcare Asset Management Second EditionNoch keine Bewertungen
- Confidentiality and Legal Components of TelemedicineDokument6 SeitenConfidentiality and Legal Components of TelemedicinegagansrikankaNoch keine Bewertungen
- Risk Assessment Advice Sheets PDFDokument16 SeitenRisk Assessment Advice Sheets PDFvishali sethiNoch keine Bewertungen
- A17 Associate Contracts England and Wales - Apr11Dokument21 SeitenA17 Associate Contracts England and Wales - Apr11nignig100% (1)
- Apollo Hospitals - BOMA Scope - UH BangladeshDokument14 SeitenApollo Hospitals - BOMA Scope - UH BangladeshHamayet RaselNoch keine Bewertungen
- Dental Service Marketing: Journal of International Oral Health September 2018Dokument5 SeitenDental Service Marketing: Journal of International Oral Health September 2018SkAliHassanNoch keine Bewertungen
- BDA Consent 2016Dokument9 SeitenBDA Consent 2016KandiwapaNoch keine Bewertungen
- Dental Hygiene ProposalDokument9 SeitenDental Hygiene Proposalmoses njengaNoch keine Bewertungen
- SDCEP Cleaning of Dental Instruments 2nd Edition Jan2016Dokument34 SeitenSDCEP Cleaning of Dental Instruments 2nd Edition Jan2016DrSukesh Upare Phd100% (1)
- Week 4 - Critical Thinking Case StudyDokument5 SeitenWeek 4 - Critical Thinking Case StudyTonya JohnsonNoch keine Bewertungen
- DentalDokument37 SeitenDentalAmanda BrunerNoch keine Bewertungen
- National Health Plan-Ministry of Health Solomon IslandsDokument29 SeitenNational Health Plan-Ministry of Health Solomon IslandsMalefoasiNoch keine Bewertungen
- Delivering Better Oral HealthDokument102 SeitenDelivering Better Oral Healthsavrasx100% (1)
- Vitamin CDokument18 SeitenVitamin CMarcel Gloria PongendaNoch keine Bewertungen
- Name of Presentation 1Dokument22 SeitenName of Presentation 1nsen69Noch keine Bewertungen
- Course Outline (Principlal Marketing EMBA - szabIST UniDokument7 SeitenCourse Outline (Principlal Marketing EMBA - szabIST UniSalman HaiderNoch keine Bewertungen
- Maintaining StandardsDokument90 SeitenMaintaining StandardsSara Loureiro da LuzNoch keine Bewertungen
- (P1) BioethicsDokument100 Seiten(P1) BioethicsGeralyn KaeNoch keine Bewertungen
- Interview Form HCADokument4 SeitenInterview Form HCAThabo NkomoNoch keine Bewertungen
- Dental Hygiene Portfolio GuideDokument12 SeitenDental Hygiene Portfolio GuideMostafa FayadNoch keine Bewertungen
- Dental Foundation Training Portfolio User GuideDokument56 SeitenDental Foundation Training Portfolio User GuideEdgar PalmaNoch keine Bewertungen
- 5.5c Infection Control Annual Work Plan 2013-14Dokument8 Seiten5.5c Infection Control Annual Work Plan 2013-14Tianti PuadiNoch keine Bewertungen
- Clinical GovernanceDokument9 SeitenClinical GovernanceSajid Rahman100% (1)
- Tulsa Memorial Hospital, Santa FE Healthcare, Copperline HealthcareDokument4 SeitenTulsa Memorial Hospital, Santa FE Healthcare, Copperline Healthcarealka murarka50% (2)
- Infection Control BDADokument15 SeitenInfection Control BDAMariam WaseemNoch keine Bewertungen
- The Concept of Access: Definition and Relationship To Consumer SatisfactionDokument15 SeitenThe Concept of Access: Definition and Relationship To Consumer SatisfactionTate SimbaNoch keine Bewertungen
- Delivering Better Oral HealthDokument102 SeitenDelivering Better Oral HealthAvina Anin NasiaNoch keine Bewertungen
- Legal and Ethical Issues HandoutDokument6 SeitenLegal and Ethical Issues HandoutKath SicatNoch keine Bewertungen
- Caries and Quality of Life in Portuguese Adolescents: Impact of Diet and Behavioural Risk FactorsDokument6 SeitenCaries and Quality of Life in Portuguese Adolescents: Impact of Diet and Behavioural Risk FactorsCristian OneaNoch keine Bewertungen
- Professional Competencies For Pharmacist Abu HabiDokument14 SeitenProfessional Competencies For Pharmacist Abu HabiIndra PratamaNoch keine Bewertungen
- Assignment History TakingDokument4 SeitenAssignment History Takinghajar4933Noch keine Bewertungen
- UW Health Strategic PlanDokument7 SeitenUW Health Strategic PlandrahmedneoNoch keine Bewertungen
- 2016 Revised Standards For Clinical Dental Hygiene PracticeDokument16 Seiten2016 Revised Standards For Clinical Dental Hygiene PracticeElvira PurnamasariNoch keine Bewertungen
- KMR FinalDokument73 SeitenKMR FinalTazeen KhanNoch keine Bewertungen
- Dental Mechanic Hand BookDokument44 SeitenDental Mechanic Hand BookARUN SAMNoch keine Bewertungen
- Medical EmergenciesDokument28 SeitenMedical EmergenciesmyletterbagNoch keine Bewertungen
- Telling The Optometrist About Me FormDokument7 SeitenTelling The Optometrist About Me FormInclusionNorthNoch keine Bewertungen
- Dental Manager Job DescriptionDokument2 SeitenDental Manager Job DescriptionSaad Hassan SyedNoch keine Bewertungen
- Safe Sedation Practice For Healthcare Procedures: Standards and GuidanceDokument39 SeitenSafe Sedation Practice For Healthcare Procedures: Standards and GuidanceAlaa ShnienNoch keine Bewertungen
- Guide To Infection Prevention in Outpatient Settings: Minimum Expectations For Safe CareDokument16 SeitenGuide To Infection Prevention in Outpatient Settings: Minimum Expectations For Safe CareJun AnteolaNoch keine Bewertungen
- Complaint HandlingDokument15 SeitenComplaint HandlingjarodzeeNoch keine Bewertungen
- Aspen Healthcare Online Interview QuestionDokument5 SeitenAspen Healthcare Online Interview QuestionNad DionisioNoch keine Bewertungen
- Infection Prevention Checklist For Dental Setting - CDCDokument20 SeitenInfection Prevention Checklist For Dental Setting - CDCDewi Ratna Sari100% (1)
- Dental Foundation Training Curriculum 2016Dokument46 SeitenDental Foundation Training Curriculum 2016Rajitha Dilhan100% (1)
- Master of Science in Health Sciences in Health Care Quality UGWDokument17 SeitenMaster of Science in Health Sciences in Health Care Quality UGWsarahNoch keine Bewertungen
- A New Drug-Shelf Arrangement For Reducing MedicatiDokument9 SeitenA New Drug-Shelf Arrangement For Reducing MedicatiEmmanuel LawerNoch keine Bewertungen
- VA 2010 2014 Strategic PlanDokument112 SeitenVA 2010 2014 Strategic PlanmaxwizeNoch keine Bewertungen
- Public Health Approaches To Prevention of Oral DiseasesDokument94 SeitenPublic Health Approaches To Prevention of Oral DiseasesZerida ZainalNoch keine Bewertungen
- Dental and Medical History FormDokument1 SeiteDental and Medical History FormBon QuiapoNoch keine Bewertungen
- Senior Medical Equipment Planner in Atlanta GA Resume Dale PalmerDokument2 SeitenSenior Medical Equipment Planner in Atlanta GA Resume Dale PalmerDalePalmerNoch keine Bewertungen
- Healthcare ErgonomicsDokument39 SeitenHealthcare Ergonomicsiqmal_faisalNoch keine Bewertungen
- 205 Principles of SafeguardingDokument16 Seiten205 Principles of SafeguardingUnCalatorNoch keine Bewertungen
- Special DeliveryDokument15 SeitenSpecial Deliveryapi-461978440Noch keine Bewertungen
- JC 2011 TRACERS Final PDFDokument38 SeitenJC 2011 TRACERS Final PDFpathoslmc globalNoch keine Bewertungen
- Breastfeeding Posters and DisplaysDokument3 SeitenBreastfeeding Posters and DisplaysDhea Rizky Amelia SatoNoch keine Bewertungen
- Comparison of Apple and Samsung LaptopDokument8 SeitenComparison of Apple and Samsung LaptopHassan AnwarNoch keine Bewertungen
- Health InsuranceDokument28 SeitenHealth InsuranceVikramaditya MuralidharanNoch keine Bewertungen
- PreschoolerDokument3 SeitenPreschoolerRetno KartikaNoch keine Bewertungen
- PreadolescentDokument1 SeitePreadolescentRetno KartikaNoch keine Bewertungen
- AdolescentDokument1 SeiteAdolescentRetno KartikaNoch keine Bewertungen
- Timeline PDDM SemgizDokument13 SeitenTimeline PDDM SemgizRetno KartikaNoch keine Bewertungen
- Taguig City UniversityDokument10 SeitenTaguig City UniversityRoy CabarlesNoch keine Bewertungen
- Kern County 2001-02 Grand Jury, Final ReportDokument169 SeitenKern County 2001-02 Grand Jury, Final ReportRick ThomaNoch keine Bewertungen
- Competing Through SustainabilityDokument4 SeitenCompeting Through SustainabilitySean SimNoch keine Bewertungen
- DAR Memo-65-S14Dokument4 SeitenDAR Memo-65-S14ceejayeNoch keine Bewertungen
- I° Medio - Lesson 1 - SolucionarioDokument10 SeitenI° Medio - Lesson 1 - SolucionarioVivianaNoch keine Bewertungen
- Letter ADokument3 SeitenLetter Amarvin kyerehNoch keine Bewertungen
- Scope of WorkDokument18 SeitenScope of WorkEric James L. PinaraNoch keine Bewertungen
- Strategic Management ºA Case Study of AppleDokument8 SeitenStrategic Management ºA Case Study of AppleDee MavreshkoNoch keine Bewertungen
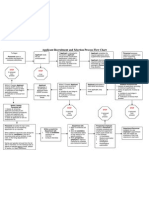
- Applicant Recruitment and Selection Flow ChartDokument1 SeiteApplicant Recruitment and Selection Flow Chartants_ramsNoch keine Bewertungen
- Private ComDokument3 SeitenPrivate ComAkjm Abdul KadirNoch keine Bewertungen
- MGT-351 Human Resource Management Chapter-1, LS/ Topic: 1Dokument15 SeitenMGT-351 Human Resource Management Chapter-1, LS/ Topic: 1Shadman Sakib FahimNoch keine Bewertungen
- P.thamarai Selvan - Updated Resume 2Dokument3 SeitenP.thamarai Selvan - Updated Resume 2rajasekar_tceNoch keine Bewertungen
- BPO DONE Group 1 Written ReportDokument7 SeitenBPO DONE Group 1 Written ReportClaire OperañaNoch keine Bewertungen
- Loan Forgiveness For Public Service EmployeesDokument2 SeitenLoan Forgiveness For Public Service EmployeesAnu Beginning ProductionzNoch keine Bewertungen
- Artech Infosystems PVT LTD Background Verification FormDokument7 SeitenArtech Infosystems PVT LTD Background Verification FormThiyagesh DhandapaniNoch keine Bewertungen
- JMM Promotion and MNGT, Inc Vs CA GR No 120096, 8-5-1996Dokument5 SeitenJMM Promotion and MNGT, Inc Vs CA GR No 120096, 8-5-1996Plinky De GuzmanNoch keine Bewertungen
- Skill Based PayDokument23 SeitenSkill Based PayAdriana GarciaNoch keine Bewertungen
- PaySlip of JanuaryDokument1 SeitePaySlip of JanuaryBharat YadavNoch keine Bewertungen
- Krishna MishragkpDokument2 SeitenKrishna MishragkpKrishna MishraNoch keine Bewertungen
- merSETA Annual Report 2021 - 22Dokument112 SeitenmerSETA Annual Report 2021 - 22Kennedy K TshegofatsoNoch keine Bewertungen
- Modern Labor Economics: The Demand For LaborDokument42 SeitenModern Labor Economics: The Demand For LaborsamuelNoch keine Bewertungen
- MBA+Project Quality+of+Work+Life (1) .Dokument60 SeitenMBA+Project Quality+of+Work+Life (1) .Divya Ram100% (1)
- Week 7-Human Resources Theories of Motivation LeadershipDokument28 SeitenWeek 7-Human Resources Theories of Motivation Leadershipcpcervantes2842antNoch keine Bewertungen
- Report MCBDokument29 SeitenReport MCBalisha waheedNoch keine Bewertungen
- Directory: MarketplaceDokument19 SeitenDirectory: MarketplaceKarthik ReddyNoch keine Bewertungen
- Marilyn Cormack To RetireDokument3 SeitenMarilyn Cormack To RetireBHcareNoch keine Bewertungen
- Reference Check FormDokument3 SeitenReference Check Formkrystelsmalls100% (2)
- Volkschel Labor Union vs. BLR, G.R. No. L-45824 (June 19, 1985)Dokument1 SeiteVolkschel Labor Union vs. BLR, G.R. No. L-45824 (June 19, 1985)Jolynne Anne GaticaNoch keine Bewertungen
- Human Resource ManagementDokument101 SeitenHuman Resource ManagementAbhishek Kumar0% (1)
- Federal Ministry of Labour and EmploymentDokument12 SeitenFederal Ministry of Labour and EmploymentPhilip Ngbede OkawuNoch keine Bewertungen