Das könnte Ihnen auch gefallen
- Adolescent Acne Vulgaris Consultant For Pediatricians Feb. 2015 PDFDokument3 SeitenAdolescent Acne Vulgaris Consultant For Pediatricians Feb. 2015 PDFDesi RatnaningtyasNoch keine Bewertungen
- Jurnal Stress OksidatifDokument8 SeitenJurnal Stress OksidatifDesi RatnaningtyasNoch keine Bewertungen
- Patch Test DrugDokument9 SeitenPatch Test DrugDesi RatnaningtyasNoch keine Bewertungen
- Antioxidants 06 00095Dokument11 SeitenAntioxidants 06 00095Desi RatnaningtyasNoch keine Bewertungen
- UV Radiation and Skin PDFDokument27 SeitenUV Radiation and Skin PDFDesi RatnaningtyasNoch keine Bewertungen
- Management of Cutaneous ErythrasmaDokument11 SeitenManagement of Cutaneous ErythrasmaDesi RatnaningtyasNoch keine Bewertungen
- Diagnosis of Common, Benign Neonatal Dermatoses: Daniel Wallach, MDDokument5 SeitenDiagnosis of Common, Benign Neonatal Dermatoses: Daniel Wallach, MDDesi RatnaningtyasNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Surigao Del Sur State University: Review of Related LiteratureDokument9 SeitenSurigao Del Sur State University: Review of Related LiteraturePrincess Marcelhyn VillegasNoch keine Bewertungen
- Awareness On HepatitisDokument52 SeitenAwareness On HepatitisMizanur RahmanNoch keine Bewertungen
- ENG 114 Medical Terminology Module 23-24Dokument47 SeitenENG 114 Medical Terminology Module 23-24zainablovebhNoch keine Bewertungen
- Pharmacologic ClassDokument4 SeitenPharmacologic ClassBianca Nicole Gacad FernandezNoch keine Bewertungen
- MOH DHA HAAD Dental Study Material Part 2Dokument33 SeitenMOH DHA HAAD Dental Study Material Part 2Junaid Ramzan89% (37)
- Gujarat Technological University: W.E.F. AY 2017-18Dokument3 SeitenGujarat Technological University: W.E.F. AY 2017-18raj royelNoch keine Bewertungen
- IMNCI Management of Childhood Illness Chart Booklet WHO 2018Dokument54 SeitenIMNCI Management of Childhood Illness Chart Booklet WHO 2018IgweNoch keine Bewertungen
- Jurnal HPLC KromatografiDokument8 SeitenJurnal HPLC KromatografiDevi AtikahNoch keine Bewertungen
- ACTD Rev.1 Part IV Clinical DocumentDokument50 SeitenACTD Rev.1 Part IV Clinical DocumentRaeanne SabadoNoch keine Bewertungen
- Role of DOAC in The Management of COVID-19 Patients: Desak Nyoman Desy LestariDokument32 SeitenRole of DOAC in The Management of COVID-19 Patients: Desak Nyoman Desy Lestaridesy lestariNoch keine Bewertungen
- Screening For Osteoporosis - UpToDateDokument22 SeitenScreening For Osteoporosis - UpToDatesindy suarezNoch keine Bewertungen
- Grand Coaching: Medical Surgical NursingDokument22 SeitenGrand Coaching: Medical Surgical NursingEsarpy (Nana)Noch keine Bewertungen
- Urinary Tract Infection, Complicated (UTI) - Johns Hopkins ABX GuideDokument5 SeitenUrinary Tract Infection, Complicated (UTI) - Johns Hopkins ABX GuideLaoMed plusNoch keine Bewertungen
- Sympathomimetics 2023 MCQDokument12 SeitenSympathomimetics 2023 MCQHossam MohamedNoch keine Bewertungen
- 12 Letter WordsDokument494 Seiten12 Letter Wordstrakds0% (1)
- 121220190CNS StimulantsDokument23 Seiten121220190CNS StimulantsHemantNoch keine Bewertungen
- Skelton Et Al-2015-Cochrane Database of Systematic ReviewsDokument30 SeitenSkelton Et Al-2015-Cochrane Database of Systematic ReviewsDamian MarreroNoch keine Bewertungen
- Bhanga 3Dokument35 SeitenBhanga 3Shanmugam PiramanayagamNoch keine Bewertungen
- Brochure TSMU - GeorgiaDokument9 SeitenBrochure TSMU - GeorgiashahulNoch keine Bewertungen
- BLUEPRINT - Basic Principles of Toxicology Elective TYDokument2 SeitenBLUEPRINT - Basic Principles of Toxicology Elective TYDAMBALENoch keine Bewertungen
- HAADDokument52 SeitenHAADElsayed AbdallahNoch keine Bewertungen
- CefuroximeDokument2 SeitenCefuroximeAngel CatalanNoch keine Bewertungen
- Drug Abuse Among The Students: June 2015Dokument8 SeitenDrug Abuse Among The Students: June 2015MohdAlifAbdullahNoch keine Bewertungen
- CHAPTER8Dokument21 SeitenCHAPTER8SankaraSatyadevNoch keine Bewertungen
- Digoxin (Lanoxin) : Routes of Administration Methods For Iv Administration and DosageDokument2 SeitenDigoxin (Lanoxin) : Routes of Administration Methods For Iv Administration and Dosageiamlx2Noch keine Bewertungen
- Review Article: Thymoma in Myasthenia Gravis: From Diagnosis To TreatmentDokument6 SeitenReview Article: Thymoma in Myasthenia Gravis: From Diagnosis To TreatmentHeru SigitNoch keine Bewertungen
- Azole Antifungals HandoutDokument8 SeitenAzole Antifungals Handoutapi-648714317Noch keine Bewertungen
- M6 Pharmaceutical LabelsDokument23 SeitenM6 Pharmaceutical Labelscbun22222Noch keine Bewertungen
- Coverage Midterm Examination 2021 Drug and Vice ControlDokument4 SeitenCoverage Midterm Examination 2021 Drug and Vice ControlTaga Phase 7Noch keine Bewertungen
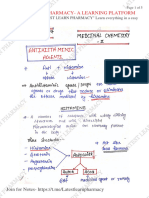
- L 1 Unit 1 Medicinal Chemistry LL LATEST LEARN PHARMACYDokument5 SeitenL 1 Unit 1 Medicinal Chemistry LL LATEST LEARN PHARMACYYASH DESHMUKH 66Noch keine Bewertungen