Das könnte Ihnen auch gefallen
- 7x Premature EjaculationDokument8 Seiten7x Premature EjaculationTer AbNoch keine Bewertungen
- Astringent Herbs Stambhana KarmaDokument4 SeitenAstringent Herbs Stambhana Karmaqueencel100% (1)
- 52 Healing HabitsDokument11 Seiten52 Healing Habitsjethro123_69Noch keine Bewertungen
- Laparoscopic CholecystectomyDokument7 SeitenLaparoscopic CholecystectomyYellow CarterNoch keine Bewertungen
- Guidelines Management of Common Bile Duct StonesDokument70 SeitenGuidelines Management of Common Bile Duct StonesMuhammad Abukhater100% (2)
- Case Study of Bronchial Asthma in Acute ExacerbationDokument16 SeitenCase Study of Bronchial Asthma in Acute Exacerbationdextroid1290% (29)
- Hypertension CASE STUDYDokument30 SeitenHypertension CASE STUDYKaloy Kamao100% (7)
- Obstructive Jaundice: Abdel Rahman A. Al Manasra, MDDokument56 SeitenObstructive Jaundice: Abdel Rahman A. Al Manasra, MDAmyandNoch keine Bewertungen
- The Guide To The Future of Medicine White PaperDokument25 SeitenThe Guide To The Future of Medicine White PaperJose Avila100% (4)
- Achytherapy 3HAXAPDokument464 SeitenAchytherapy 3HAXAPIkang FauziNoch keine Bewertungen
- Open CholecystectomyDokument35 SeitenOpen CholecystectomywqNoch keine Bewertungen
- Examination of Orthopedic and Athletic Injuries Starkey PDFDokument2 SeitenExamination of Orthopedic and Athletic Injuries Starkey PDFJenny0% (4)
- Intraoperative CholangiographyDokument6 SeitenIntraoperative CholangiographyPolly LombardiniNoch keine Bewertungen
- Management of Common Bile Duct Stones at A Tertiary Care HospitalDokument5 SeitenManagement of Common Bile Duct Stones at A Tertiary Care Hospitalindex PubNoch keine Bewertungen
- Cambio de Laparoscopia A Cirugia AbiertaDokument7 SeitenCambio de Laparoscopia A Cirugia AbiertaJosé David Cortez Centeno 20190155Noch keine Bewertungen
- Exploración VBDokument24 SeitenExploración VBEstefania Van der VazcomNoch keine Bewertungen
- 10 1016@j Suc 2018 12 007Dokument24 Seiten10 1016@j Suc 2018 12 007Gabriel RangelNoch keine Bewertungen
- 12 BuenoDokument7 Seiten12 BuenoFlipNoch keine Bewertungen
- Advantages of Laparoscopic Common Bile Duct Exploration in Common Bile Duct StonesDokument5 SeitenAdvantages of Laparoscopic Common Bile Duct Exploration in Common Bile Duct Stonesnaili nsnNoch keine Bewertungen
- 1 s2.0 S0016510796700986 Main PDFDokument8 Seiten1 s2.0 S0016510796700986 Main PDFErikson SipayungNoch keine Bewertungen
- Cierre Primario ColédocoDokument6 SeitenCierre Primario Colédocoava0311Noch keine Bewertungen
- Kenny 2014Dokument5 SeitenKenny 2014Ángel AranaNoch keine Bewertungen
- Clinical Spotlight Review For The Management of CholedocholithiasisDokument10 SeitenClinical Spotlight Review For The Management of CholedocholithiasisLourdes MarquezNoch keine Bewertungen
- Cholecystectomy and Common Bile Duct ExplorationDokument22 SeitenCholecystectomy and Common Bile Duct ExplorationmohamedhazemelfollNoch keine Bewertungen
- Cholelithiasis With Choledocholithiasis: Epidemiological, Clinical ProfileDokument3 SeitenCholelithiasis With Choledocholithiasis: Epidemiological, Clinical ProfileShashank KumarNoch keine Bewertungen
- JurnalDokument6 SeitenJurnalAgamMayzulfiNoch keine Bewertungen
- International Journal of Surgery Open: Tariq Al-Aubaidi, Basim R. Ghadhban, Samer S. ChitheerDokument7 SeitenInternational Journal of Surgery Open: Tariq Al-Aubaidi, Basim R. Ghadhban, Samer S. Chitheersamer falconNoch keine Bewertungen
- 9 Management of Common Bile-Duct Stones and Associated Gallbladder Stones: Surgical AspectsDokument14 Seiten9 Management of Common Bile-Duct Stones and Associated Gallbladder Stones: Surgical AspectsekoNoch keine Bewertungen
- Clinical Spotlight Review - Management of Choledocholithiasis - A SAGES PublicationDokument15 SeitenClinical Spotlight Review - Management of Choledocholithiasis - A SAGES PublicationMu TelaNoch keine Bewertungen
- GRP2009 840208Dokument12 SeitenGRP2009 840208Java YukiNoch keine Bewertungen
- Is It Necessary To Ligate Distal Common Bile Duct Stumps After Excising Choledochal Cysts?Dokument4 SeitenIs It Necessary To Ligate Distal Common Bile Duct Stumps After Excising Choledochal Cysts?Rajarshi KumarNoch keine Bewertungen
- Bahasa IndonesiaDokument4 SeitenBahasa IndonesiaNadiah Umniati SyarifahNoch keine Bewertungen
- Jurnal 2Dokument13 SeitenJurnal 2goldenday_hdpNoch keine Bewertungen
- The Value of MRCPDokument5 SeitenThe Value of MRCPBella YulandaNoch keine Bewertungen
- EUS: A Meta-Analysis of Test Performance in Suspected CholedocholithiasisDokument10 SeitenEUS: A Meta-Analysis of Test Performance in Suspected Choledocholithiasismphil.rameshNoch keine Bewertungen
- Accuracy of ASGE Criteria For The Prediction of Choledocholithiasis 2016Dokument6 SeitenAccuracy of ASGE Criteria For The Prediction of Choledocholithiasis 2016DannyNoch keine Bewertungen
- Is Intraoperative Cholangiography Necessary During Laparoscopic Cholecystectomy For Cholelithiasis?Dokument16 SeitenIs Intraoperative Cholangiography Necessary During Laparoscopic Cholecystectomy For Cholelithiasis?Rendy NunuhituNoch keine Bewertungen
- Diagnostic Imaging Pathways ArticleDokument9 SeitenDiagnostic Imaging Pathways ArticleIndra PrimaNoch keine Bewertungen
- MGM tắc mật không rõ nguyên nhânDokument7 SeitenMGM tắc mật không rõ nguyên nhânNguyễn Mạnh CườngNoch keine Bewertungen
- Approach Calculos Wjge 6 32 PDFDokument10 SeitenApproach Calculos Wjge 6 32 PDFJavier Alonso Jara CánovasNoch keine Bewertungen
- 2017 Updated Guideline On The Management of Common Bile Duct Stones CBDSDokument19 Seiten2017 Updated Guideline On The Management of Common Bile Duct Stones CBDSFieska AzizahNoch keine Bewertungen
- Serology and Ultrasound For Diagnosis of Choledocolitiasis 2014Dokument5 SeitenSerology and Ultrasound For Diagnosis of Choledocolitiasis 2014DannyNoch keine Bewertungen
- Role of Cholecystectomy inDokument10 SeitenRole of Cholecystectomy inLuz BecerraNoch keine Bewertungen
- Jsls 14 2 246Dokument5 SeitenJsls 14 2 246Maman SulaemanNoch keine Bewertungen
- Pie 2018Dokument5 SeitenPie 2018Tina HerreraNoch keine Bewertungen
- 10.1007@s11605 018 04090 ZDokument11 Seiten10.1007@s11605 018 04090 ZGabriel RangelNoch keine Bewertungen
- Choledocholithiasis: Evolving Standards For Diagnosis and ManagementDokument6 SeitenCholedocholithiasis: Evolving Standards For Diagnosis and ManagementAngel Princëzza LovërzNoch keine Bewertungen
- 2017 Article 3322Dokument7 Seiten2017 Article 3322Kevin MandakNoch keine Bewertungen
- Cancer de HigadoDokument8 SeitenCancer de HigadoLuis G. Moscoso ArpasiNoch keine Bewertungen
- Predictors of Failure of Endoscopic Retrograde Cholangiography in Clearance of Bile Duct Stones On Initial Procedure: A Moroccan Retrospective StudyDokument4 SeitenPredictors of Failure of Endoscopic Retrograde Cholangiography in Clearance of Bile Duct Stones On Initial Procedure: A Moroccan Retrospective StudyIJAR JOURNALNoch keine Bewertungen
- Research Article: Characteristics of Patients With Colonic Polyps Requiring Segmental ResectionDokument7 SeitenResearch Article: Characteristics of Patients With Colonic Polyps Requiring Segmental ResectionAkiko Syawalidhany TahirNoch keine Bewertungen
- Acute Transient Hepatocellular Injury in Cholelithiasis and Cholecystitis Without Evidence of CholedocholithiasisDokument5 SeitenAcute Transient Hepatocellular Injury in Cholelithiasis and Cholecystitis Without Evidence of CholedocholithiasisardytawaradaniNoch keine Bewertungen
- International Journal of Surgery: Original ResearchDokument9 SeitenInternational Journal of Surgery: Original ResearchrejNoch keine Bewertungen
- Klatskin Tumor 2Dokument8 SeitenKlatskin Tumor 2Florian JeffNoch keine Bewertungen
- Evidencia 1Dokument6 SeitenEvidencia 1Ricardo Uzcategui ArreguiNoch keine Bewertungen
- Prediction of Difficulties in Laparoscopic Cholecystectomy On The Base of Routinely Available Parameters in A Smaller Regional HospitalDokument8 SeitenPrediction of Difficulties in Laparoscopic Cholecystectomy On The Base of Routinely Available Parameters in A Smaller Regional Hospitalagha_niceNoch keine Bewertungen
- Complete Resolution of Nonalcoholic Fatty LiverDokument32 SeitenComplete Resolution of Nonalcoholic Fatty LiverRegir KurNoch keine Bewertungen
- Liver Test Patterns in Patients With Acute Calculous Cholecystitis and or CholedocholithiasisDokument8 SeitenLiver Test Patterns in Patients With Acute Calculous Cholecystitis and or Choledocholithiasismari3312Noch keine Bewertungen
- Bitcoin DiscussionDokument6 SeitenBitcoin Discussionmrpoopy123Noch keine Bewertungen
- Choledocholithiasis: Prevalence IncidenceDokument9 SeitenCholedocholithiasis: Prevalence IncidenceMike GNoch keine Bewertungen
- 012011SCNA3Dokument14 Seiten012011SCNA3mariafmhNoch keine Bewertungen
- Cytoreductive Surgery and IntraperitonealDokument11 SeitenCytoreductive Surgery and IntraperitonealJorge FallasNoch keine Bewertungen
- WJGS 8 376Dokument7 SeitenWJGS 8 376Inamullah FurqanNoch keine Bewertungen
- Csendes1992 FR Predictores de ColangitisDokument4 SeitenCsendes1992 FR Predictores de ColangitisSebastian Sapiain GonzalezNoch keine Bewertungen
- Ev 12 2020 04 AG - 5359 0562Dokument6 SeitenEv 12 2020 04 AG - 5359 0562Saran RalucaNoch keine Bewertungen
- 5 3 27 103Dokument6 Seiten5 3 27 103Khaled MonazeaNoch keine Bewertungen
- BR J Haematol - 2016 - Chaganti - Guidelines For The Management of Diffuse Large B Cell LymphomaDokument14 SeitenBR J Haematol - 2016 - Chaganti - Guidelines For The Management of Diffuse Large B Cell LymphomaAdil EissaNoch keine Bewertungen
- Endoscopy in Liver DiseaseVon EverandEndoscopy in Liver DiseaseJohn N. PlevrisNoch keine Bewertungen
- CPG Manage CholesterolDokument3 SeitenCPG Manage CholesterolShaoran AuliaNoch keine Bewertungen
- Analysis of The Degree of Undertreatment of Hyperlipidemia and Congestive Heart Failure Secondary To Coronary Artery DiseaseDokument5 SeitenAnalysis of The Degree of Undertreatment of Hyperlipidemia and Congestive Heart Failure Secondary To Coronary Artery DiseaseShaoran AuliaNoch keine Bewertungen
- Cardiac Biomarkers: When To Test? - Physician Perspective: Review ArticleDokument5 SeitenCardiac Biomarkers: When To Test? - Physician Perspective: Review ArticleShaoran AuliaNoch keine Bewertungen
- Ferdhany Effendi (Malaysia)Dokument5 SeitenFerdhany Effendi (Malaysia)Shaoran AuliaNoch keine Bewertungen
- Journal ReadingDokument23 SeitenJournal ReadingShaoran AuliaNoch keine Bewertungen
- Ddtank Play Ddtank Champions and Other Free Games Instantly in Your Favorite Web Browser. Yuk Main DdtankDokument1 SeiteDdtank Play Ddtank Champions and Other Free Games Instantly in Your Favorite Web Browser. Yuk Main DdtankShaoran AuliaNoch keine Bewertungen
- Daftar Pustaka: Liver Physiol 290:G505-G510, 2006Dokument2 SeitenDaftar Pustaka: Liver Physiol 290:G505-G510, 2006Shaoran AuliaNoch keine Bewertungen
- 17-Laboratory Evaluation of Urinary TR Act Infection v1 - 3Dokument33 Seiten17-Laboratory Evaluation of Urinary TR Act Infection v1 - 3Shaoran AuliaNoch keine Bewertungen
- Sample Size PilotDokument5 SeitenSample Size PilotmsriramcaNoch keine Bewertungen
- A Ryan Case StudyDokument6 SeitenA Ryan Case StudycryziaNoch keine Bewertungen
- Video Game TreatmentDokument1 SeiteVideo Game TreatmentYosi FestaNoch keine Bewertungen
- CP ON PUD (1) ADokument20 SeitenCP ON PUD (1) ADeekshitha DanthuluriNoch keine Bewertungen
- Stress Burnout - Georgeann RoudebushDokument45 SeitenStress Burnout - Georgeann RoudebushVinnyYusrainiNoch keine Bewertungen
- Cholera & DysenteryDokument28 SeitenCholera & DysenterySherbaz Sheikh100% (1)
- Patient CounsellingDokument19 SeitenPatient CounsellingchivconNoch keine Bewertungen
- Systems of Psychotherapy A Transtheoretical Analysis 8th Edition Prochaska Test BankDokument13 SeitenSystems of Psychotherapy A Transtheoretical Analysis 8th Edition Prochaska Test Bankmonicamartinezaekngtcimj100% (15)
- What Is Septic ShockDokument6 SeitenWhat Is Septic Shocksalome carpioNoch keine Bewertungen
- EpulisDokument7 SeitenEpulisSean Anderson100% (1)
- GPT PresentationDokument13 SeitenGPT Presentationrempit76Noch keine Bewertungen
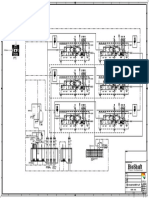
- P&ID - STP-Yanbu SWCC (6units)Dokument1 SeiteP&ID - STP-Yanbu SWCC (6units)Ashraf BayomiNoch keine Bewertungen
- Lymphoma HandoutDokument5 SeitenLymphoma Handoutapi-244850728Noch keine Bewertungen
- Foods That Can Purify Blood Naturally - PositiveMedffDokument7 SeitenFoods That Can Purify Blood Naturally - PositiveMedfftmk1989Noch keine Bewertungen
- Laporan Master Tarif Pelayanan Rawat Jalan: Kode Nama TindakanDokument9 SeitenLaporan Master Tarif Pelayanan Rawat Jalan: Kode Nama TindakanRetna Wahyu WulandariNoch keine Bewertungen
- Drug Study For HELLP SyndromeDokument19 SeitenDrug Study For HELLP SyndromeRosemarie CarpioNoch keine Bewertungen
- HMR QuestionnaireDokument7 SeitenHMR QuestionnairetrruptipatescribdNoch keine Bewertungen
- Episiotomy and SuturingDokument5 SeitenEpisiotomy and SuturingAnila SajeshNoch keine Bewertungen
- Ileocecal ResectionDokument12 SeitenIleocecal ResectionPVP BOSNIANoch keine Bewertungen
- Pre Analytical Clot EdDokument12 SeitenPre Analytical Clot EdAnonymous w4qodCJNoch keine Bewertungen
- Assertiveness Training A Forgotten EvideDokument20 SeitenAssertiveness Training A Forgotten EvideinicelliNoch keine Bewertungen
- CARDOSO Et Al 2010 - Propolis Staphylo e Malassezia - Otite CaninaDokument3 SeitenCARDOSO Et Al 2010 - Propolis Staphylo e Malassezia - Otite CaninaDébora SakiyamaNoch keine Bewertungen