Das könnte Ihnen auch gefallen
- SLEDokument42 SeitenSLETrishenth FonsekaNoch keine Bewertungen
- 17 Eman EtalDokument8 Seiten17 Eman EtaleditorijmrhsNoch keine Bewertungen
- Journal - Lung Function Changes in Young Obese Women - A Harbinger For Graver OutcomesDokument6 SeitenJournal - Lung Function Changes in Young Obese Women - A Harbinger For Graver OutcomesSondang Farwaty SitanggangNoch keine Bewertungen
- Correlation of Obesity Indices With Peak Expiratory Flow Rate in Males and FemalesDokument7 SeitenCorrelation of Obesity Indices With Peak Expiratory Flow Rate in Males and FemalesIOSR Journal of PharmacyNoch keine Bewertungen
- Exercise and Sleep-Disordered Breathing: An Association Independent of Body HabitusDokument5 SeitenExercise and Sleep-Disordered Breathing: An Association Independent of Body HabitusponnuswamyvNoch keine Bewertungen
- Co-Relation Between Body Mass Index and Intraocular Pressure in AdultsDokument4 SeitenCo-Relation Between Body Mass Index and Intraocular Pressure in AdultsAngkat Prasetya Abdi NegaraNoch keine Bewertungen
- Journal 8Dokument6 SeitenJournal 8Aceking MarquezNoch keine Bewertungen
- Gastro Oesophageal RefluxDokument7 SeitenGastro Oesophageal Refluxjustifieda13Noch keine Bewertungen
- 1 s2.0 S0954611113004137 MainDokument7 Seiten1 s2.0 S0954611113004137 MainPrama GitaNoch keine Bewertungen
- Ejgm 452Dokument7 SeitenEjgm 452Andi PurnamaNoch keine Bewertungen
- Variation of PEFR With Height, Weight and Waist-Hip Ratio in Medical StudentsDokument6 SeitenVariation of PEFR With Height, Weight and Waist-Hip Ratio in Medical StudentsInternational Medical PublisherNoch keine Bewertungen
- Sleep-Disordered Breathing and Mortality: A Prospective Cohort StudyDokument3 SeitenSleep-Disordered Breathing and Mortality: A Prospective Cohort StudyPreeti SainiNoch keine Bewertungen
- Body Composition Markers in Older Persons With COPD: A M A, A F, L S, V B, C M, A C, A C, E E. G, F LDokument6 SeitenBody Composition Markers in Older Persons With COPD: A M A, A F, L S, V B, C M, A C, A C, E E. G, F Lpina distefanoNoch keine Bewertungen
- Hubungan Antara Indeks Massa Tubuh (Imt)Dokument8 SeitenHubungan Antara Indeks Massa Tubuh (Imt)Davit ElfradoNoch keine Bewertungen
- 24 Ashraf Et AlDokument7 Seiten24 Ashraf Et AleditorijmrhsNoch keine Bewertungen
- Hakala2000 PDFDokument7 SeitenHakala2000 PDFVanshika GuptaNoch keine Bewertungen
- Valeriaceci Journal Editor 18 Degirmenci 6043Dokument8 SeitenValeriaceci Journal Editor 18 Degirmenci 6043naomigabeNoch keine Bewertungen
- Physical Activity: and Self in Cystic FibrosisDokument6 SeitenPhysical Activity: and Self in Cystic FibrosisSerian AdrianNoch keine Bewertungen
- Exercise Dose and Quality of Life: A Randomized Controlled TrialDokument10 SeitenExercise Dose and Quality of Life: A Randomized Controlled TrialThamires BarbosaNoch keine Bewertungen
- Dietary Counselling and Food Fortification in Stable COPD: A Randomised TrialDokument7 SeitenDietary Counselling and Food Fortification in Stable COPD: A Randomised TrialJames Cojab SacalNoch keine Bewertungen
- The Correlation Between Insulin Resistance and Left Ventricular Systolic Function in Obese WomenDokument4 SeitenThe Correlation Between Insulin Resistance and Left Ventricular Systolic Function in Obese WomenAgus MahendraNoch keine Bewertungen
- Restrictive Spirometry Pattern Is Associated With Low Physical Activity Levels. A Population Based International Study - ScienceDirectDokument22 SeitenRestrictive Spirometry Pattern Is Associated With Low Physical Activity Levels. A Population Based International Study - ScienceDirectSrilatha GirishNoch keine Bewertungen
- Jurnal Etiologi (EBM)Dokument9 SeitenJurnal Etiologi (EBM)Dewi LarasatiNoch keine Bewertungen
- Coping and Quality of Life in Patients Awaiting Lung TransplantationDokument21 SeitenCoping and Quality of Life in Patients Awaiting Lung TransplantationHelenaNoch keine Bewertungen
- Manuskrip Heri Gunawan Univmed English FinalDokument16 SeitenManuskrip Heri Gunawan Univmed English FinalHera HeraNoch keine Bewertungen
- 1 s2.0 S1807593222027120 MainDokument6 Seiten1 s2.0 S1807593222027120 MainPrama GitaNoch keine Bewertungen
- ICU JournalDokument2 SeitenICU JournalPau Hipol MadriagaNoch keine Bewertungen
- CARDIO METABOLIC RISK FACTORS AMONG POSTMENOPAUSAL SUDANESE WOMEN 17oct (1) Revision-TrackedDokument28 SeitenCARDIO METABOLIC RISK FACTORS AMONG POSTMENOPAUSAL SUDANESE WOMEN 17oct (1) Revision-Trackedhadiqa.iq95Noch keine Bewertungen
- Article HUNT Model For VO2peakDokument20 SeitenArticle HUNT Model For VO2peakAntonio JairoNoch keine Bewertungen
- International Journal of Pharma and Bio Sciences: Research Article Human PhysiologyDokument6 SeitenInternational Journal of Pharma and Bio Sciences: Research Article Human PhysiologyajenggayatriNoch keine Bewertungen
- 3 - Q of Life 2004Dokument6 Seiten3 - Q of Life 2004Victoria PredaNoch keine Bewertungen
- Sleep Quality and The Metabolic Syndrome: The Role of Sleep Duration and LifestyleDokument10 SeitenSleep Quality and The Metabolic Syndrome: The Role of Sleep Duration and LifestyleRegina GamezNoch keine Bewertungen
- International Journal of Pharma and Bio SciencesDokument6 SeitenInternational Journal of Pharma and Bio SciencesAdeess AengNoch keine Bewertungen
- Nin Research Paperon DiabetesDokument4 SeitenNin Research Paperon DiabetesAvantikaNoch keine Bewertungen
- Internasional Jurnal Aerobik 4Dokument11 SeitenInternasional Jurnal Aerobik 4Lala NobitaNoch keine Bewertungen
- Anthropometrical Parameters Are Not Related With Lipid Profile in Mild To Moderate AsthmaDokument5 SeitenAnthropometrical Parameters Are Not Related With Lipid Profile in Mild To Moderate AsthmaOpenaccess Research paperNoch keine Bewertungen
- Senam Bugar Lansia Berpengaruh Terhadap Daya Tahan Jantung Paru, Status Gizi, Dan Tekanan DarahDokument9 SeitenSenam Bugar Lansia Berpengaruh Terhadap Daya Tahan Jantung Paru, Status Gizi, Dan Tekanan DarahBilal MashelNoch keine Bewertungen
- Selección de Resúmenes de Menopausia Semana Del 22 Al 28 de Octubre de 2014Dokument3 SeitenSelección de Resúmenes de Menopausia Semana Del 22 Al 28 de Octubre de 2014rocksurNoch keine Bewertungen
- Impact of Obesity On Respiratory Disorder SeverityDokument94 SeitenImpact of Obesity On Respiratory Disorder SeverityThaman ThimmaiahNoch keine Bewertungen
- Cross Sectional 1Dokument7 SeitenCross Sectional 1Ridho KurniaNoch keine Bewertungen
- Effect of Practicing Deep Breathing Exercise On Improving Quality of Life of Gastroesophageal Reflux Disease PatientsDokument14 SeitenEffect of Practicing Deep Breathing Exercise On Improving Quality of Life of Gastroesophageal Reflux Disease PatientsMita AmaliaNoch keine Bewertungen
- Selección de Resúmenes de Menopausia Semana Del 10 Al 21 de Septiembre de 2014Dokument5 SeitenSelección de Resúmenes de Menopausia Semana Del 10 Al 21 de Septiembre de 2014rocksurNoch keine Bewertungen
- Nutrients 12 00932 v2Dokument16 SeitenNutrients 12 00932 v2Mario CoelhoNoch keine Bewertungen
- Jurnal Massa Bebas LemakDokument10 SeitenJurnal Massa Bebas Lemakmona nurdin nurdinNoch keine Bewertungen
- Cardiopulmonary Exercise Testing in Patients With Liver CirrhosisDokument4 SeitenCardiopulmonary Exercise Testing in Patients With Liver Cirrhosistengku zadeqNoch keine Bewertungen
- Balloon TherapyDokument6 SeitenBalloon TherapyIntan NingsihNoch keine Bewertungen
- Panchami JCDR 7 1322Dokument3 SeitenPanchami JCDR 7 1322reza salzabellaNoch keine Bewertungen
- PFT PSGDokument51 SeitenPFT PSGGuenevere DamasinNoch keine Bewertungen
- Pulmonary Function Tests in Type 2 DiabetesDokument4 SeitenPulmonary Function Tests in Type 2 DiabetesIOSRjournalNoch keine Bewertungen
- Physical Activity and Mortality in Indiv PDFDokument11 SeitenPhysical Activity and Mortality in Indiv PDFYudistiraNoch keine Bewertungen
- Seminar: Amy S Jordan, David G Mcsharry, Atul MalhotraDokument12 SeitenSeminar: Amy S Jordan, David G Mcsharry, Atul MalhotraSerkan KüçüktürkNoch keine Bewertungen
- Shahad 7Dokument10 SeitenShahad 7Mohammed OmarNoch keine Bewertungen
- Capacity (FVC) Pria Dewasa Denganoverweight: Pengaruh Latihan Aerobik Terhadap Forced VitalDokument6 SeitenCapacity (FVC) Pria Dewasa Denganoverweight: Pengaruh Latihan Aerobik Terhadap Forced VitalKimbek BuangkeNoch keine Bewertungen
- Assessment of Overweight and High Blood Pressure Among Individuals in Out - Patient Clinic in A Specialist HospitalDokument3 SeitenAssessment of Overweight and High Blood Pressure Among Individuals in Out - Patient Clinic in A Specialist HospitalIOSRjournalNoch keine Bewertungen
- Research ProposalDokument10 SeitenResearch ProposalDeborahNoch keine Bewertungen
- Prevalence of Hypertension Among Obese and Non-Obese Patients With Coronary Artery DiseaseDokument4 SeitenPrevalence of Hypertension Among Obese and Non-Obese Patients With Coronary Artery DiseasePrinceTumbuktooNoch keine Bewertungen
- Nutrients: Micronutrient Status in 153 Patients With Anorexia NervosaDokument10 SeitenNutrients: Micronutrient Status in 153 Patients With Anorexia NervosaReza Yusna HanastaNoch keine Bewertungen
- Crosstalk Proposal: High Intensity Interval Training Does Have A Role in Risk Reduction or Treatment of DiseaseDokument3 SeitenCrosstalk Proposal: High Intensity Interval Training Does Have A Role in Risk Reduction or Treatment of Diseaseapi-298930008Noch keine Bewertungen
- Thorax00329 0017Dokument2 SeitenThorax00329 0017Dário Talita SantanaNoch keine Bewertungen
- Obesity and Lung Disease: A Guide to ManagementVon EverandObesity and Lung Disease: A Guide to ManagementAnne E. DixonNoch keine Bewertungen
- Complementary and Alternative Medical Lab Testing Part 2: RespiratoryVon EverandComplementary and Alternative Medical Lab Testing Part 2: RespiratoryNoch keine Bewertungen
- Case ReportDokument11 SeitenCase ReportBerhanu DigamoNoch keine Bewertungen
- PNC Checklist AfricanDokument2 SeitenPNC Checklist AfricanAudrey Andini0% (1)
- F Buski 111003095909 Phpapp01Dokument15 SeitenF Buski 111003095909 Phpapp01Ashik MajumdarNoch keine Bewertungen
- Improving VO2 Max Through ExerciseDokument1 SeiteImproving VO2 Max Through ExercisecathyNoch keine Bewertungen
- 11 Human Body SystemDokument3 Seiten11 Human Body SystemCris EnriquezNoch keine Bewertungen
- Massage Techniques and Effects PresentationDokument35 SeitenMassage Techniques and Effects Presentationama00Noch keine Bewertungen
- On and Off Male Birth Control MethodsDokument2 SeitenOn and Off Male Birth Control MethodsLeón L.PNoch keine Bewertungen
- Major Depressive Disorder Symptoms and Prevalence For IB Abnormal PsychologyDokument13 SeitenMajor Depressive Disorder Symptoms and Prevalence For IB Abnormal PsychologychrissybissyNoch keine Bewertungen
- P1 RleDokument34 SeitenP1 RleMary Jean GicaNoch keine Bewertungen
- Newborn CareDokument19 SeitenNewborn CareYa Mei LiNoch keine Bewertungen
- Ultrasound Thesis TopicsDokument6 SeitenUltrasound Thesis Topicsdw9x1bxb100% (2)
- Lesson 3 - Substance Use, Addictions, Mental Health, Stigma and Discrimination and in The WorkplaceDokument8 SeitenLesson 3 - Substance Use, Addictions, Mental Health, Stigma and Discrimination and in The WorkplaceCala WritesNoch keine Bewertungen
- Diabetes Jigsaw ActivitiesDokument11 SeitenDiabetes Jigsaw ActivitiesJacqueline CullieNoch keine Bewertungen
- HOẰNG HÓA 4-THANH HÓA 2022Dokument6 SeitenHOẰNG HÓA 4-THANH HÓA 2022Tuấn KhanhNoch keine Bewertungen
- Celiac DiseaseDokument5 SeitenCeliac DiseaseJhevey ValdezNoch keine Bewertungen
- Chorea 9Dokument35 SeitenChorea 9sanjay kamineniNoch keine Bewertungen
- MacroalbuminemiaDokument4 SeitenMacroalbuminemiailma_ilemNoch keine Bewertungen
- Abnormal Vaginal Bleeding Policar 051611Dokument69 SeitenAbnormal Vaginal Bleeding Policar 051611bidan22Noch keine Bewertungen
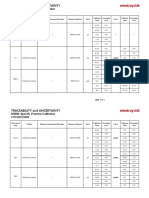
- Specific Proteins Calibrator-150721009-BS600Dokument2 SeitenSpecific Proteins Calibrator-150721009-BS600S6b2Noch keine Bewertungen
- Acute Parenchymal Liver DiseaseDokument29 SeitenAcute Parenchymal Liver Diseasejeevan ghimireNoch keine Bewertungen
- Editorial: Dental Caries and OsteoporosisDokument2 SeitenEditorial: Dental Caries and OsteoporosisBagis Emre GulNoch keine Bewertungen
- Jamaophthalmology Biswas 2016 Oi 160055Dokument8 SeitenJamaophthalmology Biswas 2016 Oi 160055Ghalia HayetNoch keine Bewertungen
- Chronic Inflammatory Demyelinating PolyradiculoneuropathyDokument5 SeitenChronic Inflammatory Demyelinating PolyradiculoneuropathyDiego Fernando AlegriaNoch keine Bewertungen
- Euthanasia in Experimental AnimalsDokument22 SeitenEuthanasia in Experimental AnimalsParmanand AtalNoch keine Bewertungen
- EpilepsyDokument38 SeitenEpilepsyJareena BegumNoch keine Bewertungen
- Physical Abuse Teaching SlidesDokument19 SeitenPhysical Abuse Teaching SlidesbentoeNoch keine Bewertungen
- Rachel Bray - ResumeDokument2 SeitenRachel Bray - Resumeapi-625221885Noch keine Bewertungen
- COVID-19 and Pregnancy: A Review of Clinical Characteristics, Obstetric Outcomes and Vertical TransmissionDokument20 SeitenCOVID-19 and Pregnancy: A Review of Clinical Characteristics, Obstetric Outcomes and Vertical TransmissionDra Sandra VèlezNoch keine Bewertungen
- Is Doa 10 Cup TestDokument1 SeiteIs Doa 10 Cup TestUqi.Noch keine Bewertungen