Das könnte Ihnen auch gefallen
- Thyroid Suppression Test With L-Thyroxine and TC) PertechnetateDokument7 SeitenThyroid Suppression Test With L-Thyroxine and TC) PertechnetatejeffsunilNoch keine Bewertungen
- ClonidineDokument4 SeitenClonidineDR RAVI ANANDNoch keine Bewertungen
- Bja 2013Dokument9 SeitenBja 2013Gihan NakhlehNoch keine Bewertungen
- Chassot 2012Dokument9 SeitenChassot 2012docadax848Noch keine Bewertungen
- 33 FullDokument5 Seiten33 FullIndahK.WardhaniPutriNoch keine Bewertungen
- Henke 2003Dokument6 SeitenHenke 2003handrionoNoch keine Bewertungen
- 3781 FullDokument6 Seiten3781 FullSukhvinder Singh RanaNoch keine Bewertungen
- Wa0010.Dokument9 SeitenWa0010.deinoterraNoch keine Bewertungen
- Early Postoperative ComplicationsDokument6 SeitenEarly Postoperative Complications49hr84j7spNoch keine Bewertungen
- Comparison of Ketamine-Midazolam-Propofol Combination and Fentanyl-Midazolam-Propofol Combination For Sedation in ColonosDokument8 SeitenComparison of Ketamine-Midazolam-Propofol Combination and Fentanyl-Midazolam-Propofol Combination For Sedation in ColonosDendy AgusNoch keine Bewertungen
- Thyroid-Hormone Concentrations After Radiolodine Therapy For HyperthyroidismDokument5 SeitenThyroid-Hormone Concentrations After Radiolodine Therapy For HyperthyroidismShane AllenNoch keine Bewertungen
- Haloperidol Combined With DexamethasoneDokument6 SeitenHaloperidol Combined With Dexamethasoneapi-741687858Noch keine Bewertungen
- Seo2016 PDFDokument8 SeitenSeo2016 PDFNovia AyuNoch keine Bewertungen
- dst50234 PDFDokument7 Seitendst50234 PDFtaniaNoch keine Bewertungen
- HyperthyroidDokument7 SeitenHyperthyroidHaerun Nisa SiregarNoch keine Bewertungen
- Remifentanil Compared With Midazolam and Pethidine Sedation During Colonoscopy: A Prospective, Randomized StudyDokument7 SeitenRemifentanil Compared With Midazolam and Pethidine Sedation During Colonoscopy: A Prospective, Randomized Studyade_liaNoch keine Bewertungen
- The Analgesic Efficacy of Tramadol As A Pre-Emptive Analgesic in Pediatric Appendectomy Patients PDFDokument6 SeitenThe Analgesic Efficacy of Tramadol As A Pre-Emptive Analgesic in Pediatric Appendectomy Patients PDFUmmu Qonitah AfnidawatiNoch keine Bewertungen
- The Effects of Age On Neural Blockade and Hemodynamic Changes After Epidural Anesthesia With RopivacaineDokument6 SeitenThe Effects of Age On Neural Blockade and Hemodynamic Changes After Epidural Anesthesia With RopivacaineAnonymous K9tmd7T0PzNoch keine Bewertungen
- Annals of International Medical and Dental ResearchDokument4 SeitenAnnals of International Medical and Dental ResearchDr Rohit varshneyNoch keine Bewertungen
- Retroperitoneal MassDokument22 SeitenRetroperitoneal Massapi-434838777Noch keine Bewertungen
- Hellp 2Dokument7 SeitenHellp 2Nur Rahmat WibowoNoch keine Bewertungen
- Adrenal Insufficiency in Thyroid Cancer Patients Treated With Tyrosine Kinase Inhibitors and Detected by ACTH Stimulation TestDokument9 SeitenAdrenal Insufficiency in Thyroid Cancer Patients Treated With Tyrosine Kinase Inhibitors and Detected by ACTH Stimulation TestEmanuel CalderonNoch keine Bewertungen
- Artikel Mathemathical Model Graves DiseaseDokument12 SeitenArtikel Mathemathical Model Graves DiseaseFreija GeldofNoch keine Bewertungen
- Prevention of Shivering During Regional Anaesthesia - Comparison of Midazolam, Midazolam Plus Ketamine, Tramadol, and Tramadol Plus KetamineDokument17 SeitenPrevention of Shivering During Regional Anaesthesia - Comparison of Midazolam, Midazolam Plus Ketamine, Tramadol, and Tramadol Plus Ketamineandi ananNoch keine Bewertungen
- Ajrccm 163 1 16310aDokument3 SeitenAjrccm 163 1 16310amisulica2010Noch keine Bewertungen
- Jurnal AnastesiDokument5 SeitenJurnal AnastesiNadya Tenriany NajibNoch keine Bewertungen
- Randomised Trial of Corticosteroids in The of Tuberculous PleurisyDokument4 SeitenRandomised Trial of Corticosteroids in The of Tuberculous PleurisyDrVinod Kumar Goud VemulaNoch keine Bewertungen
- Taprogge Et Al 2021 A Systematic Review and Meta Analysis of The Relationship Between The Radiation Absorbed Dose ToDokument10 SeitenTaprogge Et Al 2021 A Systematic Review and Meta Analysis of The Relationship Between The Radiation Absorbed Dose ToLesly LoachamínNoch keine Bewertungen
- Personalized Dosimetry in Diagnostic and Therapeutic Nuclear MedicineDokument34 SeitenPersonalized Dosimetry in Diagnostic and Therapeutic Nuclear MedicineRafa PopocaNoch keine Bewertungen
- Adherence To Oral Hypoglycemic MedicatioDokument20 SeitenAdherence To Oral Hypoglycemic Medicatioashenafi woldesenbetNoch keine Bewertungen
- 2014-Effects and Mechanisms of Transcutaneous Electroacupuncture On Chemotherapy Induced Nausea and VomitingDokument6 Seiten2014-Effects and Mechanisms of Transcutaneous Electroacupuncture On Chemotherapy Induced Nausea and VomitingvictoregvNoch keine Bewertungen
- The Hemodynamic Effects of Propofol in Children With Congenital Heart DiseaseDokument6 SeitenThe Hemodynamic Effects of Propofol in Children With Congenital Heart DiseaseAngelica Lucero OrtizNoch keine Bewertungen
- 2010 Stuard Pycnogenol Improves Kidney Function in Metabolic SyndromeDokument6 Seiten2010 Stuard Pycnogenol Improves Kidney Function in Metabolic Syndromeindoglo1Noch keine Bewertungen
- Journal 2Dokument6 SeitenJournal 2chaNoch keine Bewertungen
- 701 2011 Article 959Dokument9 Seiten701 2011 Article 959Kumaran Bagavathi RagavanNoch keine Bewertungen
- 20Dokument9 Seiten20Amina GoharyNoch keine Bewertungen
- Dome-And-Dart T Waves and Hyperthyroidism - A Case ReportDokument3 SeitenDome-And-Dart T Waves and Hyperthyroidism - A Case ReportMiftah MiftahNoch keine Bewertungen
- Dysphagia: Impact On Quality of Life After Radio (Chemo) Therapy of Head and Neck CancerDokument7 SeitenDysphagia: Impact On Quality of Life After Radio (Chemo) Therapy of Head and Neck CancerNurul Afika LubisNoch keine Bewertungen
- Sedation For Fibreoptic Gastroscopy: A Comparative Study of Midazolam and DiazepamDokument8 SeitenSedation For Fibreoptic Gastroscopy: A Comparative Study of Midazolam and DiazepamRomaNoch keine Bewertungen
- JCO 2005 Pink 6809 11Dokument3 SeitenJCO 2005 Pink 6809 11claudiaNoch keine Bewertungen
- NIH Public Access: Author ManuscriptDokument10 SeitenNIH Public Access: Author ManuscriptNurci Efrilia SafitriNoch keine Bewertungen
- AMPT-induced Monoamine Depletion in Humans: Evaluation of Two Alternative (123I) IBZM SPECT ProceduresDokument7 SeitenAMPT-induced Monoamine Depletion in Humans: Evaluation of Two Alternative (123I) IBZM SPECT ProceduresMihaela ToaderNoch keine Bewertungen
- Radio Active Iodine Ablation in Well Differentiated Thyroid Cancers 2155 9619.1000e103Dokument1 SeiteRadio Active Iodine Ablation in Well Differentiated Thyroid Cancers 2155 9619.1000e103Yola Ivonny HariantoNoch keine Bewertungen
- Jcem2157 PDFDokument6 SeitenJcem2157 PDFRidwan Putra Beng-BengNoch keine Bewertungen
- Jurnal AnastesiaDokument8 SeitenJurnal AnastesiaFikri SatriaNoch keine Bewertungen
- 00003Dokument8 Seiten00003Anonymous zPwXqwNoch keine Bewertungen
- Nice SugarDokument15 SeitenNice SugarRafaela LealNoch keine Bewertungen
- A Double Blind, Randomised, Controlled Trial To Study The Effect of Dexmeditomidine On Hemodynamic and Recovery Responses During Tracheal ExtubationDokument8 SeitenA Double Blind, Randomised, Controlled Trial To Study The Effect of Dexmeditomidine On Hemodynamic and Recovery Responses During Tracheal ExtubationramukolakiNoch keine Bewertungen
- Rogers 1993Dokument4 SeitenRogers 1993Nadia SaiNoch keine Bewertungen
- Consevative RX of AnDokument6 SeitenConsevative RX of AnMusthafa Afif WardhanaNoch keine Bewertungen
- AJCC6 TH Ed Cancer Staging Manual Part 1Dokument8 SeitenAJCC6 TH Ed Cancer Staging Manual Part 1handrionoNoch keine Bewertungen
- 689 FullDokument5 Seiten689 FullBlu TuxNoch keine Bewertungen
- Reports of Practical Oncology and Radiotherapy 1 8 (2 0 1 3) S186-S197Dokument2 SeitenReports of Practical Oncology and Radiotherapy 1 8 (2 0 1 3) S186-S197Elisa SalakayNoch keine Bewertungen
- Hemodynamic Effects of Chest-Knee Position: Comparison of Perioperative Propofol and Sevoflurane AnesthesiaDokument6 SeitenHemodynamic Effects of Chest-Knee Position: Comparison of Perioperative Propofol and Sevoflurane AnesthesiaAprilico Fadhil PangestuNoch keine Bewertungen
- Comparison of The Efficacy of Propofol TCI and Midazolam For Patients Undergoing ESWL - RCTDokument5 SeitenComparison of The Efficacy of Propofol TCI and Midazolam For Patients Undergoing ESWL - RCTharvardboyNoch keine Bewertungen
- Consensus and Controversy of Radioiodine and PET (Or Pet/Ct) in The Management of Well-Differentiated Thyroid CancerDokument31 SeitenConsensus and Controversy of Radioiodine and PET (Or Pet/Ct) in The Management of Well-Differentiated Thyroid CancerBosan KhalidNoch keine Bewertungen
- New Evidence in Home Mechanical Ventilation: Thematic Poster Session Hall 2-4 - 12:50-14:40Dokument5 SeitenNew Evidence in Home Mechanical Ventilation: Thematic Poster Session Hall 2-4 - 12:50-14:40Shirley CoelhoNoch keine Bewertungen
- 131I Therapy For Elevated Thyroglobulin LevelsDokument8 Seiten131I Therapy For Elevated Thyroglobulin LevelsMeutia sariNoch keine Bewertungen
- TraztuzumabDokument8 SeitenTraztuzumabArlina Wiyata GamaNoch keine Bewertungen
- Introduction To Parasitology & Lab Diagnosis of ParasiticDokument33 SeitenIntroduction To Parasitology & Lab Diagnosis of ParasiticMaharRkpNoch keine Bewertungen
- Cell Structures Part One: Roxanne Ferguson Biology Graves County High SchoolDokument13 SeitenCell Structures Part One: Roxanne Ferguson Biology Graves County High SchoolMaharRkpNoch keine Bewertungen
- Functional Expressions Starting The CommunicationDokument7 SeitenFunctional Expressions Starting The CommunicationMaharRkpNoch keine Bewertungen
- 6 Adjective ClauseDokument16 Seiten6 Adjective ClauseMaharRkpNoch keine Bewertungen
- 8 Functional ExpressionsDokument35 Seiten8 Functional ExpressionsMaharRkpNoch keine Bewertungen
- 10 AbbreviationDokument5 Seiten10 AbbreviationMaharRkpNoch keine Bewertungen
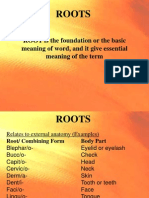
- Roots: ROOT Is The Foundation or The Basic Meaning of Word, and It Give Essential Meaning of The TermDokument4 SeitenRoots: ROOT Is The Foundation or The Basic Meaning of Word, and It Give Essential Meaning of The TermMaharRkpNoch keine Bewertungen
- Cell VocabularyDokument18 SeitenCell VocabularyMaharRkpNoch keine Bewertungen
- Mitosis and The Cell CycleDokument27 SeitenMitosis and The Cell CycleMaharRkpNoch keine Bewertungen
- Mutasi Gonosom ManusiaDokument20 SeitenMutasi Gonosom ManusiaMaharRkpNoch keine Bewertungen
- Cell Structures Lesson2Dokument12 SeitenCell Structures Lesson2MaharRkpNoch keine Bewertungen
- Cell Division: MeiosisDokument16 SeitenCell Division: MeiosisMaharRkpNoch keine Bewertungen
- Roots: ROOT Is The Foundation or The Basic Meaning of Word, and It Give Essential Meaning of The TermDokument4 SeitenRoots: ROOT Is The Foundation or The Basic Meaning of Word, and It Give Essential Meaning of The TermMaharRkpNoch keine Bewertungen
- 6 Adjective ClauseDokument16 Seiten6 Adjective ClauseMaharRkp100% (1)
- A Comparison of The Revised Delirium Rating ScaleDokument8 SeitenA Comparison of The Revised Delirium Rating ScaleMaharRkpNoch keine Bewertungen
- English of NursingDokument6 SeitenEnglish of NursingMaharRkpNoch keine Bewertungen
- Pengaruh Deep Back Massage Terhadap Penurunan NyeriDokument14 SeitenPengaruh Deep Back Massage Terhadap Penurunan NyeriMaharRkpNoch keine Bewertungen
- Uv DoseDokument6 SeitenUv DoseRajesh DeshmukhNoch keine Bewertungen
- Aceclofenac Vs Diclofenac On Hexosamine LevelsDokument11 SeitenAceclofenac Vs Diclofenac On Hexosamine LevelsMartin MoranNoch keine Bewertungen
- PlacentaDokument21 SeitenPlacentaAttiqaQureshiNoch keine Bewertungen
- Klinefelters SyndromeDokument2 SeitenKlinefelters SyndromeAlexandra Gabriella ZawisnyNoch keine Bewertungen
- Grade 4 Chondromalacia Patella TreatmentDokument3 SeitenGrade 4 Chondromalacia Patella TreatmentTroy0% (1)
- 2 Articles From Oui Magazine (Feat. Robert Anton Wilson)Dokument16 Seiten2 Articles From Oui Magazine (Feat. Robert Anton Wilson)Jakob AndradeNoch keine Bewertungen
- Form 4 Medical Certificate For Non-Gazetted Officer Recommended For Leave or Extension or Commutation of LeaveDokument2 SeitenForm 4 Medical Certificate For Non-Gazetted Officer Recommended For Leave or Extension or Commutation of LeaveDr RajaNoch keine Bewertungen
- Refeeding SyndromeDokument10 SeitenRefeeding SyndromePhysiology by Dr RaghuveerNoch keine Bewertungen
- Order of Payment: Food and Drug AdministrationDokument2 SeitenOrder of Payment: Food and Drug AdministrationTheGood GuyNoch keine Bewertungen
- CeftriaxoneDokument2 SeitenCeftriaxoneFlora Angeli PastoresNoch keine Bewertungen
- A Systematic Review of Trunk Restraint TrainingDokument1 SeiteA Systematic Review of Trunk Restraint Traininggans_therapist3321Noch keine Bewertungen
- AJODO-90 Petrovic Et Al Role of The Lateral Pterigoid Muscle and Menisco Temporomandibular...Dokument12 SeitenAJODO-90 Petrovic Et Al Role of The Lateral Pterigoid Muscle and Menisco Temporomandibular...ortodoncia 2018Noch keine Bewertungen
- Medical Laboratory Technology Journal: Potensi Antifungi Tangkai Daun Jarak Pagar Terhadap PERTUMBUHAN Candida AlbicansDokument5 SeitenMedical Laboratory Technology Journal: Potensi Antifungi Tangkai Daun Jarak Pagar Terhadap PERTUMBUHAN Candida Albicanskhoko holicNoch keine Bewertungen
- WC500059147 PDFDokument140 SeitenWC500059147 PDFAnaStankovićNoch keine Bewertungen
- Case Study - DR EldaDokument3 SeitenCase Study - DR EldaShashi KumarNoch keine Bewertungen
- Neuroshield ReportDokument2 SeitenNeuroshield Reportrahim pathanNoch keine Bewertungen
- Case Study 103Dokument8 SeitenCase Study 103Jonah MaasinNoch keine Bewertungen
- Pediatric Meningitis Case StudyDokument5 SeitenPediatric Meningitis Case StudyCheska PalomaNoch keine Bewertungen
- Una Coales-Get Through Medical School - 1000 Sbas Bofs and Emqs (Get Through Series) (2003) PDFDokument151 SeitenUna Coales-Get Through Medical School - 1000 Sbas Bofs and Emqs (Get Through Series) (2003) PDFCathy QianNoch keine Bewertungen
- Metatron Resonance Brochure WebsiteDokument3 SeitenMetatron Resonance Brochure WebsiteShaun DennisNoch keine Bewertungen
- Pre-Diabetes:: Don't Let It Lead To Type-2Dokument1 SeitePre-Diabetes:: Don't Let It Lead To Type-2ARIA MINDNoch keine Bewertungen
- Service Manual 2008-10-09 SP1Dokument116 SeitenService Manual 2008-10-09 SP1brunorafoNoch keine Bewertungen
- Physiotherapy in DementiaDokument4 SeitenPhysiotherapy in DementiaNabilla Yuharlina100% (1)
- PMLS 2 LEC Module 3Dokument8 SeitenPMLS 2 LEC Module 3Peach DaquiriNoch keine Bewertungen
- Romsons All ProductDokument53 SeitenRomsons All ProductBoyke WinterbergNoch keine Bewertungen
- Writing Letters of RecommendationDokument4 SeitenWriting Letters of Recommendationwenskyrose1100% (1)
- Case Study AnalysisDokument13 SeitenCase Study Analysisapi-317809407Noch keine Bewertungen
- Orthodontics!!Dokument9 SeitenOrthodontics!!Ayesha AwanNoch keine Bewertungen
- Saccharothrixsp Abh26 PDFDokument7 SeitenSaccharothrixsp Abh26 PDFAlia RahmaNoch keine Bewertungen