Das könnte Ihnen auch gefallen
- Pone. EbolaDokument12 SeitenPone. EbolaJuan MoralesNoch keine Bewertungen
- ResearchDokument11 SeitenResearchdon yenNoch keine Bewertungen
- WJH 3 130bacteremiaDokument7 SeitenWJH 3 130bacteremiaLasiaf AlaskaNoch keine Bewertungen
- Recent Advances in The Development and Evaluation of Molecular Diagnostics For Evola Virus DiseaseDokument30 SeitenRecent Advances in The Development and Evaluation of Molecular Diagnostics For Evola Virus DiseaseWendi IochNoch keine Bewertungen
- Incidence of Primary Opportunistic Infections in Two Human Immunodeficiency Virus-Infected French Clinical CohortsDokument30 SeitenIncidence of Primary Opportunistic Infections in Two Human Immunodeficiency Virus-Infected French Clinical Cohortsputri1114Noch keine Bewertungen
- Research ArticleDokument7 SeitenResearch ArticleFikri SatriaNoch keine Bewertungen
- Thypoid PDFDokument7 SeitenThypoid PDFOmy Ning PratiwiNoch keine Bewertungen
- JPAM Vol 14 Issue1 P 609-614Dokument6 SeitenJPAM Vol 14 Issue1 P 609-614Tira Alfiani LaariyaNoch keine Bewertungen
- Posters: A Sample of 156 of 232 Nurses Answered An Anonymous QuestionDokument7 SeitenPosters: A Sample of 156 of 232 Nurses Answered An Anonymous QuestionFiras DrNoch keine Bewertungen
- Invasive Fungal Sinusitis in Patients With Hematological Malignancy: 15 Years Experience in A Single University Hospital in TaiwanDokument9 SeitenInvasive Fungal Sinusitis in Patients With Hematological Malignancy: 15 Years Experience in A Single University Hospital in TaiwanAngelin LigiantoNoch keine Bewertungen
- Seminars in Diagnostic Pathology: Review ArticleDokument4 SeitenSeminars in Diagnostic Pathology: Review ArticlePradeep TandonNoch keine Bewertungen
- De-Escalation of Antimicrobial Treatment in Neutropenic Patients With Severe Sepsis: Results From An Observational StudyDokument10 SeitenDe-Escalation of Antimicrobial Treatment in Neutropenic Patients With Severe Sepsis: Results From An Observational StudyyostiNoch keine Bewertungen
- Mortality & Recurrent Seizure Risk After New-Onset Seizure in HIV-positive Zambian AdultsDokument10 SeitenMortality & Recurrent Seizure Risk After New-Onset Seizure in HIV-positive Zambian AdultsAdam PrabataNoch keine Bewertungen
- Ebola Virus Disease PDFDokument31 SeitenEbola Virus Disease PDFBibiqnaNoch keine Bewertungen
- EbolaDokument9 SeitenEbolaMara MoránNoch keine Bewertungen
- Invasive Fungal Infections in Pediatric Oncology: MD MD MD MD MD MDDokument6 SeitenInvasive Fungal Infections in Pediatric Oncology: MD MD MD MD MD MDerickmattosNoch keine Bewertungen
- Epidemiology of Recurrent Hand, Foot and Mouth Disease, China, 2008-2015Dokument11 SeitenEpidemiology of Recurrent Hand, Foot and Mouth Disease, China, 2008-2015Catherine BasinNoch keine Bewertungen
- Medical Mycology Case ReportsDokument4 SeitenMedical Mycology Case ReportsSebastián Garay HuertasNoch keine Bewertungen
- Toaidj 5 9 PDFDokument8 SeitenToaidj 5 9 PDFDini WurnaningNoch keine Bewertungen
- Epstein-Barr Virus-Related Post-Transplant Lymphoproliferative Disorder in Solid Organ Transplant RecipientsDokument10 SeitenEpstein-Barr Virus-Related Post-Transplant Lymphoproliferative Disorder in Solid Organ Transplant Recipients19112281s3785Noch keine Bewertungen
- Acinetobacter Baumannii in Ventilator-Associated PneumoniaDokument8 SeitenAcinetobacter Baumannii in Ventilator-Associated PneumoniaMahmoudAboAlSamenNoch keine Bewertungen
- Kaforou 2013Dokument18 SeitenKaforou 2013Ellyana PerwitasariNoch keine Bewertungen
- Prognostic Factors in Tuberculosis Related Mortalities in Hospitalized PatientsDokument7 SeitenPrognostic Factors in Tuberculosis Related Mortalities in Hospitalized PatientsAshok PanjwaniNoch keine Bewertungen
- AIDS Research and Therapy Volume 10 Issue 1 2013 (Doi 10.1186/1742-6405!10!16) Henry Namme Luma, Benjamin Clet Nguenkam Tchaleu - Tuberculous Meningitis - Presentation, Diagnosis and Outcome in HivDokument6 SeitenAIDS Research and Therapy Volume 10 Issue 1 2013 (Doi 10.1186/1742-6405!10!16) Henry Namme Luma, Benjamin Clet Nguenkam Tchaleu - Tuberculous Meningitis - Presentation, Diagnosis and Outcome in HivBilly Shan LastKagerooboroNoch keine Bewertungen
- Knowledge, Attitudes, and Practices (KAP) of Healthcare Workers On Viral Hepatitis B and Its Vaccination in 12 Health Establishments in The Centre Region of CameroonDokument8 SeitenKnowledge, Attitudes, and Practices (KAP) of Healthcare Workers On Viral Hepatitis B and Its Vaccination in 12 Health Establishments in The Centre Region of CameroonInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- A Prospective Study of Tuberculosis and Human Immunodeficiency Virus Infection Clinical Manifestations and Factors Associated With SurvivalDokument8 SeitenA Prospective Study of Tuberculosis and Human Immunodeficiency Virus Infection Clinical Manifestations and Factors Associated With SurvivalAbrahamKatimeNoch keine Bewertungen
- Tamiflu and Use in Coronavirus (COVID-19)Dokument3 SeitenTamiflu and Use in Coronavirus (COVID-19)zoransohridNoch keine Bewertungen
- Undiagnosed Tuberculosis in Patients With HIV Infection Who Present With Severe Anaemia at A District HospitalDokument6 SeitenUndiagnosed Tuberculosis in Patients With HIV Infection Who Present With Severe Anaemia at A District HospitalDian EsthyNoch keine Bewertungen
- Malaria Vs DBDDokument9 SeitenMalaria Vs DBDade hajizah br ritongaNoch keine Bewertungen
- Prevalence and Determinants of Human Immunodeficiency Virus and Tuberculosis Co-Infection at Kampala International University Teaching HospitalDokument6 SeitenPrevalence and Determinants of Human Immunodeficiency Virus and Tuberculosis Co-Infection at Kampala International University Teaching HospitalKIU PUBLICATION AND EXTENSIONNoch keine Bewertungen
- Ijmsv02p0050 PDFDokument8 SeitenIjmsv02p0050 PDFfikaanugrahNoch keine Bewertungen
- Multi-Country Monkeypox Outbreak - Situation UpdateDokument12 SeitenMulti-Country Monkeypox Outbreak - Situation UpdateDita Odylia DitaNoch keine Bewertungen
- Prevalencia de Infecciones Bacterianas Por Gérmenes Oportunistas o Comunes en PVVSDokument10 SeitenPrevalencia de Infecciones Bacterianas Por Gérmenes Oportunistas o Comunes en PVVSJuan Carlos ValenciaNoch keine Bewertungen
- tmp7F77 TMPDokument9 Seitentmp7F77 TMPFrontiersNoch keine Bewertungen
- Infection Is Acommonproblem ForDokument11 SeitenInfection Is Acommonproblem ForDitaMayasariNoch keine Bewertungen
- Khvi 15 10 1649532Dokument17 SeitenKhvi 15 10 1649532bilou hertNoch keine Bewertungen
- Taccone2015 Article EpidemiologyOfInvasiveAspergilDokument15 SeitenTaccone2015 Article EpidemiologyOfInvasiveAspergilsafaridikaNoch keine Bewertungen
- Sande's HIV - AIDS Medicine (PDFDrive)Dokument562 SeitenSande's HIV - AIDS Medicine (PDFDrive)angel muñozNoch keine Bewertungen
- 0074 0276 Mioc 109 01 00118Dokument4 Seiten0074 0276 Mioc 109 01 00118Luis Gabriel Parra LaraNoch keine Bewertungen
- Case Report Plasmodium Vivax Infected PatientDokument8 SeitenCase Report Plasmodium Vivax Infected Patientjohanna monsalveNoch keine Bewertungen
- Ebola VirusDokument14 SeitenEbola Virusrama hanggara dNoch keine Bewertungen
- Nosocomial Bloodstream Infection and Clinical SepsisDokument6 SeitenNosocomial Bloodstream Infection and Clinical SepsiswintannNoch keine Bewertungen
- Henze2022 Article ManagementOfHerpesvirusReactivDokument21 SeitenHenze2022 Article ManagementOfHerpesvirusReactivXXXI-JKhusnan Mustofa GufronNoch keine Bewertungen
- HZVDokument15 SeitenHZVMarviane ThenNoch keine Bewertungen
- mc7 Impact of HIV and AIDS On Surgical PracticeDokument5 Seitenmc7 Impact of HIV and AIDS On Surgical PracticeRichard EscalonaNoch keine Bewertungen
- Prevalence and Drug Resistance of Nontuberculous Mycobacteria, Northern China, 2008-2011Dokument2 SeitenPrevalence and Drug Resistance of Nontuberculous Mycobacteria, Northern China, 2008-2011Mark ReinhardtNoch keine Bewertungen
- 2016 Article 1849 PDFDokument8 Seiten2016 Article 1849 PDFdydy_7193Noch keine Bewertungen
- 1 s2.0 S1876034119303375 MainDokument6 Seiten1 s2.0 S1876034119303375 MainJuliana Menara de Souza MarquesNoch keine Bewertungen
- Diagnosis & Treatment of Tuberculosis in HIV Co-Infected PatientsDokument16 SeitenDiagnosis & Treatment of Tuberculosis in HIV Co-Infected PatientsdevisilalahiNoch keine Bewertungen
- Ofab 174Dokument4 SeitenOfab 174MarioNoch keine Bewertungen
- 2953 Hbsag SkriningDokument4 Seiten2953 Hbsag Skriningursula 002Noch keine Bewertungen
- Epidemiology, Treatment and Prevention of Healthcare-Associated Urinary Tract InfectionsDokument9 SeitenEpidemiology, Treatment and Prevention of Healthcare-Associated Urinary Tract InfectionsAnke NemirovskyNoch keine Bewertungen
- Chapter 1Dokument32 SeitenChapter 1Robee Camille Desabelle-SumatraNoch keine Bewertungen
- Jurnal Tifoid C 2Dokument12 SeitenJurnal Tifoid C 2Yulia PuspitaNoch keine Bewertungen
- Clinical Microbiology and Infection: Original ArticleDokument8 SeitenClinical Microbiology and Infection: Original ArticlePriambodo GandhiNoch keine Bewertungen
- Prevalence of Human Immunodeficiency Virus Infection Among Tuberculosis Patients at Infectious Disease Hospital, Kano State, NigeriaDokument8 SeitenPrevalence of Human Immunodeficiency Virus Infection Among Tuberculosis Patients at Infectious Disease Hospital, Kano State, NigeriaUMYU Journal of Microbiology Research (UJMR)Noch keine Bewertungen
- Ak 2011Dokument6 SeitenAk 2011bouchra8blsNoch keine Bewertungen
- 1 s2.0 S0272638620306120 ManinDokument10 Seiten1 s2.0 S0272638620306120 ManinrezaNoch keine Bewertungen
- Jurnal 6Dokument2 SeitenJurnal 6kalstarNoch keine Bewertungen
- Hepatitis B Virus and Liver DiseaseVon EverandHepatitis B Virus and Liver DiseaseJia-Horng KaoNoch keine Bewertungen
- Beef Curry Recipe - Bon AppétitDokument4 SeitenBeef Curry Recipe - Bon AppétitGunung MahameruNoch keine Bewertungen
- Adri Usg KoasDokument108 SeitenAdri Usg KoasGunung MahameruNoch keine Bewertungen
- Bucatini With Walnut-Parsley Pesto: IngredientsDokument3 SeitenBucatini With Walnut-Parsley Pesto: IngredientsGunung MahameruNoch keine Bewertungen
- Homemade Flour Tortillas - The Pioneer WomanDokument24 SeitenHomemade Flour Tortillas - The Pioneer WomanGunung MahameruNoch keine Bewertungen
- Physiology of LaborDokument49 SeitenPhysiology of LaborGunung MahameruNoch keine Bewertungen
- Dapus AdenomiosisDokument1 SeiteDapus AdenomiosisGunung MahameruNoch keine Bewertungen
- Dapus AdenomiosisDokument1 SeiteDapus AdenomiosisGunung MahameruNoch keine Bewertungen
- Dapus AdenomiosisDokument1 SeiteDapus AdenomiosisGunung MahameruNoch keine Bewertungen
- Fetal Transfusion PDFDokument4 SeitenFetal Transfusion PDFGunung MahameruNoch keine Bewertungen
- Impact of IllnessDokument34 SeitenImpact of IllnessGunung MahameruNoch keine Bewertungen
- ACLSDokument30 SeitenACLSAgilNoviarAlvirosa50% (2)
- Are Massimiliano Allegri's Record-Breakers Now Better Than The Juventus of Zinedine Zidane or Michel Platini - GoalDokument13 SeitenAre Massimiliano Allegri's Record-Breakers Now Better Than The Juventus of Zinedine Zidane or Michel Platini - GoalGunung MahameruNoch keine Bewertungen
- Adverse Effects of TransfusionDokument2 SeitenAdverse Effects of TransfusionGunung MahameruNoch keine Bewertungen
- Alternatives and Adjuncts To Blood TransfusionDokument2 SeitenAlternatives and Adjuncts To Blood TransfusionGunung MahameruNoch keine Bewertungen
- Lionel Messi On Worst Scoring Run Since 2011 - GoalDokument14 SeitenLionel Messi On Worst Scoring Run Since 2011 - GoalGunung MahameruNoch keine Bewertungen
- Transfusion Guidelines Pediatrics - Penelusuran GoogleDokument2 SeitenTransfusion Guidelines Pediatrics - Penelusuran GoogleGunung MahameruNoch keine Bewertungen
- Del Piero - No Surprise If Napoli Pip Juventus To Title - GoalDokument7 SeitenDel Piero - No Surprise If Napoli Pip Juventus To Title - GoalGunung MahameruNoch keine Bewertungen
- Juventus News - GoalDokument3 SeitenJuventus News - GoalGunung MahameruNoch keine Bewertungen
- AC Milan Unlucky To Face Sensational Buffon - Allegri - GoalDokument8 SeitenAC Milan Unlucky To Face Sensational Buffon - Allegri - GoalGunung MahameruNoch keine Bewertungen
- Activating Proliferating: Antigen Presenting CellDokument1 SeiteActivating Proliferating: Antigen Presenting CellGunung MahameruNoch keine Bewertungen
- VERRATIDokument7 SeitenVERRATIGunung MahameruNoch keine Bewertungen
- Vintage Badge in Illustrator and Photoshop - Abduzeedo Design InspirationDokument28 SeitenVintage Badge in Illustrator and Photoshop - Abduzeedo Design InspirationGunung MahameruNoch keine Bewertungen
- Pain Rating Scales: Instructions For Producing A VAS Bedside Card: Option 1Dokument4 SeitenPain Rating Scales: Instructions For Producing A VAS Bedside Card: Option 1João Ferreira da SilvaNoch keine Bewertungen
- Who PSM Par 2006.6 PDFDokument136 SeitenWho PSM Par 2006.6 PDFfathaNoch keine Bewertungen
- Findings From Britain: The Effects Illness Quality of Households in GreatDokument7 SeitenFindings From Britain: The Effects Illness Quality of Households in GreatGunung MahameruNoch keine Bewertungen
- Higher Algebra - Hall & KnightDokument593 SeitenHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Clinical Management 07Dokument22 SeitenClinical Management 07Fauzi SatriaNoch keine Bewertungen
- Evidence Based MedicineDokument22 SeitenEvidence Based MedicineLastry WardaniNoch keine Bewertungen
- Concomitant SquintDokument21 SeitenConcomitant SquintShivani NairNoch keine Bewertungen
- Pass The MRCS HistoryDokument115 SeitenPass The MRCS HistoryMariajanNoch keine Bewertungen
- Sexually Transmitted DiseaseDokument38 SeitenSexually Transmitted Diseaserana arslanNoch keine Bewertungen
- CRF Fluid Volume Excess NCPDokument3 SeitenCRF Fluid Volume Excess NCPchubbielitaNoch keine Bewertungen
- FELTP Progress Report 2020Dokument53 SeitenFELTP Progress Report 2020ehsanlarikNoch keine Bewertungen
- Rheumatoid Arthritis Drug StudyDokument2 SeitenRheumatoid Arthritis Drug StudyChristaNoch keine Bewertungen
- Immunology and Immunochemistry PDFDokument8 SeitenImmunology and Immunochemistry PDFboatcomNoch keine Bewertungen
- Gastro MCQsDokument14 SeitenGastro MCQsvaegmundigNoch keine Bewertungen
- "COVID Is Fake Sick Actually Have Influenza A or B", by Dr. Derek KnaussDokument2 Seiten"COVID Is Fake Sick Actually Have Influenza A or B", by Dr. Derek KnaussSANDRA BAGGNoch keine Bewertungen
- Benign Breast Diseases29.7Dokument65 SeitenBenign Breast Diseases29.7api-3701915Noch keine Bewertungen
- CDC - Pelvic Inflammatory Disease - 2010 STD Treatment GuidelinesDokument7 SeitenCDC - Pelvic Inflammatory Disease - 2010 STD Treatment GuidelinesAhmad Arbi AninditoNoch keine Bewertungen
- 1-4, 2016 qhd1Dokument205 Seiten1-4, 2016 qhd1waleed.almusharaf100% (1)
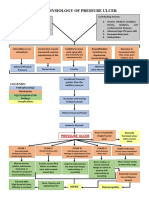
- Pathophysiology of Pressure UlcerDokument1 SeitePathophysiology of Pressure UlcerSTORAGE FILENoch keine Bewertungen
- Manual InternDokument136 SeitenManual InternalvinatNoch keine Bewertungen
- C-Reactive Protein in Serum by NephelometryDokument12 SeitenC-Reactive Protein in Serum by NephelometryTrajceNoch keine Bewertungen
- MetoprololDokument3 SeitenMetoprololapi-3797941100% (3)
- Kawasaki Disease Case ReportDokument17 SeitenKawasaki Disease Case ReportAlvaro Villarejo PérezNoch keine Bewertungen
- Neck Pain: Simple ExercisesDokument2 SeitenNeck Pain: Simple ExercisesVijaya Krishna DevarapalliNoch keine Bewertungen
- Diabetes & Stem Cell - Poster.Dokument1 SeiteDiabetes & Stem Cell - Poster.Cardio VascularNoch keine Bewertungen
- Life Is A Continous Process of AdjustmentDokument78 SeitenLife Is A Continous Process of AdjustmentGulmoharNoch keine Bewertungen
- Ventricular Septal DefectDokument16 SeitenVentricular Septal DefectPai PAiNoch keine Bewertungen
- Valvular Heart DiseaseDokument73 SeitenValvular Heart Diseaseindia2puppy100% (4)
- Combination Hyperbaric Oxygen and Temozolomide Therapy in c6 Rat Glioma ModelDokument5 SeitenCombination Hyperbaric Oxygen and Temozolomide Therapy in c6 Rat Glioma ModelDICKY PANDUWINATANoch keine Bewertungen
- RetinaDokument19 SeitenRetinaSuze C.Noch keine Bewertungen
- Vigabatrin For IsDokument12 SeitenVigabatrin For IsAndrew SantosoNoch keine Bewertungen
- Limping Child: Department of Orthopaedics Afmc, PuneDokument101 SeitenLimping Child: Department of Orthopaedics Afmc, Punerithesh ramachandranNoch keine Bewertungen
- Trauma Thoraks PDFDokument86 SeitenTrauma Thoraks PDFMiftahurrahmiNoch keine Bewertungen
- Systematic Review Pelaksanaan Programmatic Management of Drug-Resistant Tuberculosis Pada Pasien Tuberkulosis Resistan ObatDokument8 SeitenSystematic Review Pelaksanaan Programmatic Management of Drug-Resistant Tuberculosis Pada Pasien Tuberkulosis Resistan ObatAdinda Pramesthi RiadyaniNoch keine Bewertungen
- Psychiatric ScreeningDokument1 SeitePsychiatric ScreeningCatalina BorquezNoch keine Bewertungen
- NGT Ogt-FeedingDokument14 SeitenNGT Ogt-Feedingnibbles nibblesNoch keine Bewertungen