Das könnte Ihnen auch gefallen
- Good Health in the Tropics: Advice to Travellers and SettlersVon EverandGood Health in the Tropics: Advice to Travellers and SettlersNoch keine Bewertungen
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsVon EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsBewertung: 5 von 5 Sternen5/5 (9)
- Adult Pocafeket SizeDokument2 SeitenAdult Pocafeket SizedadfNoch keine Bewertungen
- Adult ScheduleDokument3 SeitenAdult ScheduledrmanojvimalNoch keine Bewertungen
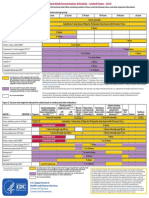
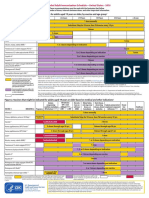
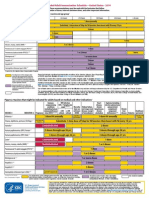
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDokument2 SeitenFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNoch keine Bewertungen
- Adult ScheduleDokument3 SeitenAdult SchedulelcmurilloNoch keine Bewertungen
- Adult Schedule 11x17Dokument2 SeitenAdult Schedule 11x17lcmurilloNoch keine Bewertungen
- Adult Combined ScheduleDokument5 SeitenAdult Combined SchedulelcmurilloNoch keine Bewertungen
- Adult Combined ScheduleDokument5 SeitenAdult Combined ScheduleAwal Safar MNoch keine Bewertungen
- Summary of Recommendations For Adult Immunization: (Age 19 Years and Older)Dokument5 SeitenSummary of Recommendations For Adult Immunization: (Age 19 Years and Older)Hannah Caburian RemoNoch keine Bewertungen
- Adult Combined Schedule VaccineDokument33 SeitenAdult Combined Schedule VaccinehatsuneNoch keine Bewertungen
- Adult ScheduleDokument3 SeitenAdult ScheduleerilarchiNoch keine Bewertungen
- Adult Combined ScheduleDokument6 SeitenAdult Combined ScheduleAstrid Elaine RosalesNoch keine Bewertungen
- Stay Healthy, Stay On Top of Vaccinations: CDC Click Here For The CDC's Full Vaccination ChartDokument4 SeitenStay Healthy, Stay On Top of Vaccinations: CDC Click Here For The CDC's Full Vaccination ChartcircularreasoningNoch keine Bewertungen
- Summary of Recommendations For Adult Immunization: (Age 19 Years & Older)Dokument4 SeitenSummary of Recommendations For Adult Immunization: (Age 19 Years & Older)gyna_2002Noch keine Bewertungen
- States, 2011 United Recommended Childhood and Adolescent Immunization SchedulesDokument7 SeitenStates, 2011 United Recommended Childhood and Adolescent Immunization SchedulesDolores KilpatrickNoch keine Bewertungen
- Recommended Immunizations FS enDokument2 SeitenRecommended Immunizations FS enirfanmajeed1987Noch keine Bewertungen
- DR Swati Rajagopal - Adult VaccinationDokument50 SeitenDR Swati Rajagopal - Adult VaccinationYabooNoch keine Bewertungen
- Vaccination Requirements and Form I-693: Mary Naughton, MD, MPHDokument55 SeitenVaccination Requirements and Form I-693: Mary Naughton, MD, MPHErinaNoch keine Bewertungen
- Immunization Routine Table1Dokument9 SeitenImmunization Routine Table1MeeKo VideñaNoch keine Bewertungen
- Standing Orders For Administering Tdap/Td To Adults: (Name of Practice or Clinic)Dokument1 SeiteStanding Orders For Administering Tdap/Td To Adults: (Name of Practice or Clinic)selvie87Noch keine Bewertungen
- Table 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenDokument8 SeitenTable 2: Summary of WHO Position Papers - Recommended Routine Immunizations For Childrenfadityo1Noch keine Bewertungen
- Immunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaDokument24 SeitenImmunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaEugene YeboahNoch keine Bewertungen
- WHO Immunization Schedule ChildrenDokument9 SeitenWHO Immunization Schedule Childrenashchua21Noch keine Bewertungen
- 1 CombineDokument726 Seiten1 CombineSong Hành Vạn KiếpNoch keine Bewertungen
- Recommended Immunization - Canadian Immunization Guide - Seventh Edition - 2006Dokument2 SeitenRecommended Immunization - Canadian Immunization Guide - Seventh Edition - 2006Maja MudriNoch keine Bewertungen
- ScheduleDokument2 SeitenScheduleapi-286634335Noch keine Bewertungen
- Table 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenDokument7 SeitenTable 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenKrishnendu PramanikNoch keine Bewertungen
- Types of ImmunizationsDokument21 SeitenTypes of Immunizationsmacmactongos100% (6)
- Adult ImmunizationDokument6 SeitenAdult ImmunizationAmit GoelNoch keine Bewertungen
- Human Papillomavirus Bivalent Vaccin1Dokument8 SeitenHuman Papillomavirus Bivalent Vaccin1alejandro fernandezNoch keine Bewertungen
- Pneumococcal Conjugate: VaccineDokument2 SeitenPneumococcal Conjugate: VaccineJenny TaylorNoch keine Bewertungen
- Vaccine Timing CDCDokument40 SeitenVaccine Timing CDCanindita.prasidha.parameswariNoch keine Bewertungen
- Expanded Program On Immunization CHNDokument4 SeitenExpanded Program On Immunization CHNgeralynroseNoch keine Bewertungen
- Expanded Program On ImmunizationDokument4 SeitenExpanded Program On ImmunizationMac Lester DumagNoch keine Bewertungen
- Ob 1.05 Clinical Practice Guidelines On Immunization For Filipino WomenDokument7 SeitenOb 1.05 Clinical Practice Guidelines On Immunization For Filipino Womenotartil_niman50% (2)
- Adult Immunization: It's Your Best Shot!Dokument40 SeitenAdult Immunization: It's Your Best Shot!minerva_stanciuNoch keine Bewertungen
- Guidelines For Vaccination in Normal Adults in India - PMCDokument14 SeitenGuidelines For Vaccination in Normal Adults in India - PMCSKMH INSURANCENoch keine Bewertungen
- Vacunas 2012Dokument7 SeitenVacunas 2012dr.alexisleon9124Noch keine Bewertungen
- Summary of Recommendations For Child Teen Immunization: (Age Birth Through 18 Years)Dokument5 SeitenSummary of Recommendations For Child Teen Immunization: (Age Birth Through 18 Years)Annie AnnaNoch keine Bewertungen
- Peace Corps MTG FOIA Volunteer Health SupportDokument199 SeitenPeace Corps MTG FOIA Volunteer Health SupportAccessible Journal Media: Peace Corps DocumentsNoch keine Bewertungen
- Epi PowerpointDokument29 SeitenEpi PowerpointFelisa Lacsamana Gregorio100% (3)
- Epi NotesDokument5 SeitenEpi NoteshoneykrizelNoch keine Bewertungen
- Current Presumptive Immunization SchedulesDokument4 SeitenCurrent Presumptive Immunization SchedulesPedro Julian Tenorio ApesteguiNoch keine Bewertungen
- Vaccinations For Adults: You're Never Too Old To Get Vaccinated!Dokument1 SeiteVaccinations For Adults: You're Never Too Old To Get Vaccinated!aliNoch keine Bewertungen
- World Immunization Week 2023 PPA EPIDokument42 SeitenWorld Immunization Week 2023 PPA EPIMuhammad ShafiNoch keine Bewertungen
- Typhoid Fever Follow-Up PDFDokument16 SeitenTyphoid Fever Follow-Up PDFPlot BUnniesNoch keine Bewertungen
- Cdi 2106 CDokument2 SeitenCdi 2106 CVerdi LeonardoNoch keine Bewertungen
- Altered Immunocompetence: UpdatesDokument27 SeitenAltered Immunocompetence: UpdatestrishnaNoch keine Bewertungen
- ImmunizationDokument40 SeitenImmunizationHilyaJae-heeNoch keine Bewertungen
- Immunization EPI Huda 201212Dokument5 SeitenImmunization EPI Huda 201212Aerish TupazNoch keine Bewertungen
- Influenza Antiviral Medications: A Summary For CliniciansDokument6 SeitenInfluenza Antiviral Medications: A Summary For CliniciansSachin S RaneNoch keine Bewertungen
- Clinical Guideline: Recommended Adult Immunization Schedule: United States, 2011Dokument8 SeitenClinical Guideline: Recommended Adult Immunization Schedule: United States, 2011Hery PriyantoNoch keine Bewertungen
- Qdenga Epar Product Information enDokument47 SeitenQdenga Epar Product Information enNovrina Wahidah RestiNoch keine Bewertungen
- Pediatric Primary CareDokument66 SeitenPediatric Primary Carefairwoods100% (1)
- VaccineDokument3 SeitenVaccinePapitas FritasNoch keine Bewertungen
- Expanded Program On ImmunizationDokument7 SeitenExpanded Program On ImmunizationGLadys Gegare100% (1)
- ImmunizationsDokument2 SeitenImmunizationsSonny KusumaNoch keine Bewertungen
- CPG On Immunization For WomenDokument28 SeitenCPG On Immunization For WomenYnoli DiosomitoNoch keine Bewertungen
- Immreq15 16Dokument2 SeitenImmreq15 16api-234991765Noch keine Bewertungen
- Drug Cal - Practice TestDokument2 SeitenDrug Cal - Practice TestBryan Mae H. DegorioNoch keine Bewertungen
- Sampling Process and Measurement ScaleDokument18 SeitenSampling Process and Measurement ScaleBryan Mae H. DegorioNoch keine Bewertungen
- Allergies or Food Intolerances.: Therapeutic DietDokument3 SeitenAllergies or Food Intolerances.: Therapeutic DietBryan Mae H. DegorioNoch keine Bewertungen
- Introduction To Change: Towards Excellence: "PHIC Accredited Health Care Provider"Dokument3 SeitenIntroduction To Change: Towards Excellence: "PHIC Accredited Health Care Provider"Bryan Mae H. DegorioNoch keine Bewertungen
- Worksheet in BloodDokument12 SeitenWorksheet in BloodBryan Mae H. DegorioNoch keine Bewertungen
- EmbryologyDokument26 SeitenEmbryologyBryan Mae H. Degorio100% (2)
- Systems of Measurement and Drug CalculationDokument13 SeitenSystems of Measurement and Drug CalculationBryan Mae H. DegorioNoch keine Bewertungen
- Preceptor Handbook For Nursing EducationDokument41 SeitenPreceptor Handbook For Nursing EducationBryan Mae H. Degorio0% (1)
- Drugs Affecting The Immune SystemDokument4 SeitenDrugs Affecting The Immune SystemBryan Mae H. DegorioNoch keine Bewertungen
- Care of Patient With Musculoskeletal DisordersDokument3 SeitenCare of Patient With Musculoskeletal DisordersBryan Mae H. DegorioNoch keine Bewertungen
- Documentation and ReportingDokument32 SeitenDocumentation and ReportingBryan Mae H. Degorio100% (1)
- Case Studies in Nursing Fundamentals - Trueman, Margaret Sorrell - Page 170-178Dokument9 SeitenCase Studies in Nursing Fundamentals - Trueman, Margaret Sorrell - Page 170-178Bryan Mae H. Degorio0% (3)
- The Adult LearningDokument15 SeitenThe Adult LearningBryan Mae H. DegorioNoch keine Bewertungen
- Is Mentorship For YOUDokument17 SeitenIs Mentorship For YOUBryan Mae H. DegorioNoch keine Bewertungen
- Key (10) Principles of CST - 1 PagerDokument1 SeiteKey (10) Principles of CST - 1 PagerBryan Mae H. DegorioNoch keine Bewertungen
- Case Studies For Bowel EliminationDokument2 SeitenCase Studies For Bowel EliminationBryan Mae H. Degorio100% (2)
- 04 Tissue, Glands and MembranesDokument52 Seiten04 Tissue, Glands and MembranesBryan Mae H. Degorio100% (1)
- Cardiac AssessmentDokument7 SeitenCardiac AssessmentBryan Mae H. Degorio75% (4)
- Shock and SIRSDokument85 SeitenShock and SIRSBryan Mae H. DegorioNoch keine Bewertungen
- Care of Patient With Nutritional and Metabolic DisordersDokument10 SeitenCare of Patient With Nutritional and Metabolic DisordersBryan Mae H. DegorioNoch keine Bewertungen
- Substance AbuseDokument32 SeitenSubstance AbuseBryan Mae H. Degorio100% (3)
- Slides For SeizureDokument15 SeitenSlides For SeizureBryan Mae H. Degorio100% (3)
- Intraoperative NursingDokument41 SeitenIntraoperative NursingBryan Mae H. Degorio100% (11)
- Psychotropic Drugs: Bryan Mae H. DegorioDokument65 SeitenPsychotropic Drugs: Bryan Mae H. DegorioBryan Mae H. Degorio100% (2)
- Case Study For Hepatitis BDokument24 SeitenCase Study For Hepatitis BEmma Mariz Bernas Garcia67% (6)
- Annex General Medical CertificateDokument1 SeiteAnnex General Medical CertificateNicole AranaNoch keine Bewertungen
- Table 44-8 Nursing Assessment: Hepatitis Subjective Data Important Health InformationDokument7 SeitenTable 44-8 Nursing Assessment: Hepatitis Subjective Data Important Health InformationAnggela kian puspaNoch keine Bewertungen
- 9 - Hepatitis B VaccineDokument1 Seite9 - Hepatitis B VaccineabhivnairNoch keine Bewertungen
- Nursing Care Plan Related Learning Experience: Lorma Colleges Con TemplateDokument2 SeitenNursing Care Plan Related Learning Experience: Lorma Colleges Con TemplateKrizzia Mae ColladoNoch keine Bewertungen
- Krok 2018 1Dokument3 SeitenKrok 2018 1Raosahab VipulyadavNoch keine Bewertungen
- HepB Provider Tipsheet 508Dokument2 SeitenHepB Provider Tipsheet 508Jamshaid AhmedNoch keine Bewertungen
- Adult Combined ScheduleDokument6 SeitenAdult Combined SchedulesharvaniNoch keine Bewertungen
- Immune and Molecular DiagnosticsDokument33 SeitenImmune and Molecular DiagnosticsManisha PorpavaiNoch keine Bewertungen
- Unknown PDFDokument56 SeitenUnknown PDFMuhammad AdiNoch keine Bewertungen
- Hepatitis B PDFDokument8 SeitenHepatitis B PDFponekNoch keine Bewertungen
- Community Medicine MCQsDokument355 SeitenCommunity Medicine MCQsKalpu Bala100% (10)
- Newborn CareDokument15 SeitenNewborn Caresupritha50% (2)
- Adult Combined ScheduleDokument10 SeitenAdult Combined ScheduledrabdulrabbNoch keine Bewertungen
- Hepatitis B Vaccine and Immunoglobulin: Key Concepts: Review ArticleDokument7 SeitenHepatitis B Vaccine and Immunoglobulin: Key Concepts: Review ArticleMarcelitaTaliaDuwiriNoch keine Bewertungen
- Injection Site and Needle Size Vaccine Dose RouteDokument1 SeiteInjection Site and Needle Size Vaccine Dose RouteDoc JT BylnNoch keine Bewertungen
- HE1446 - Hepatitis B Consent Form - 0Dokument5 SeitenHE1446 - Hepatitis B Consent Form - 0KAREEM KHANNoch keine Bewertungen
- Immunization ScheduleDokument1 SeiteImmunization ScheduleOksana PersaudNoch keine Bewertungen
- Thimerosal Content of US Vaccines 02-04Dokument3 SeitenThimerosal Content of US Vaccines 02-04Diane StierNoch keine Bewertungen
- Sample Test Questions For The CPC Exam-1Dokument6 SeitenSample Test Questions For The CPC Exam-1Anonymous MtKJkerbpU100% (2)
- Hep B VaccineDokument2 SeitenHep B VaccineLegendX100% (2)
- Novas Diretrizes Hepatite BDokument18 SeitenNovas Diretrizes Hepatite BJess jourNoch keine Bewertungen
- Insert Hep B Engerix-BDokument16 SeitenInsert Hep B Engerix-BshifanahmedNoch keine Bewertungen
- Drug StudyDokument8 SeitenDrug StudyYaniiee DeFiestaNoch keine Bewertungen
- Osce QuestionsDokument128 SeitenOsce Questionsdean100% (1)
- Epidemiology Exam Questions and AnswersDokument107 SeitenEpidemiology Exam Questions and Answersdimitrios82% (34)
- Hep B VaccineDokument2 SeitenHep B VaccineJeremy SuhardiNoch keine Bewertungen
- Expanded Program On Immunization (EPI) 7 Vaccine-Preventable Diseases VaccinesDokument7 SeitenExpanded Program On Immunization (EPI) 7 Vaccine-Preventable Diseases VaccinesLuiciaNoch keine Bewertungen
- Hepatitis Learning GuideDokument71 SeitenHepatitis Learning Guidequimico clinico 27100% (10)
- Nursery Drug Study 2 1Dokument22 SeitenNursery Drug Study 2 1Wenalyn Grace Abella LlavanNoch keine Bewertungen