Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Bab 3 Assesmen Pasien PDFDokument36 SeitenBab 3 Assesmen Pasien PDFdamartriutomoNoch keine Bewertungen
- Odontogenic Infections in The Etiology of Infective EndocarditisDokument5 SeitenOdontogenic Infections in The Etiology of Infective EndocarditiserdentNoch keine Bewertungen
- 203 202 1 PBDokument9 Seiten203 202 1 PBAji SayogoNoch keine Bewertungen
- Fracture MaxillarisDokument7 SeitenFracture MaxillarisMuhammad Arman ArraufNoch keine Bewertungen
- Treatment of Malaria-Guidelines For Clinicians WHO PDFDokument9 SeitenTreatment of Malaria-Guidelines For Clinicians WHO PDFMuhammad Arman ArraufNoch keine Bewertungen
- Treatment of Malaria-Guidelines For Clinicians WHO PDFDokument9 SeitenTreatment of Malaria-Guidelines For Clinicians WHO PDFMuhammad Arman ArraufNoch keine Bewertungen
- Malaria Diagnosis and Treatment Practices Following Introduction of Rapid Diagnostic Tests in Kibaha District, Coast Region, TanzaniaDokument8 SeitenMalaria Diagnosis and Treatment Practices Following Introduction of Rapid Diagnostic Tests in Kibaha District, Coast Region, TanzaniaMuhammad Arman ArraufNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Jennifer Marie TrenkampDokument5 SeitenJennifer Marie TrenkampJames LindonNoch keine Bewertungen
- Review Rasa SindhuraDokument9 SeitenReview Rasa SindhuraNCSASTRONoch keine Bewertungen
- NOM-073-SSA1-2015 English VersionDokument22 SeitenNOM-073-SSA1-2015 English Versionmaria najera100% (2)
- Controlled Drug DeliveryDokument23 SeitenControlled Drug DeliveryAnburaj JamesNoch keine Bewertungen
- Angela Dela Cruz-MunarrizDokument29 SeitenAngela Dela Cruz-MunarrizangelaNoch keine Bewertungen
- Effect of Hepatic and Renal Impairment On PharmacokineticDokument46 SeitenEffect of Hepatic and Renal Impairment On PharmacokineticPURVI NEEMANoch keine Bewertungen
- HMR TemplateDokument2 SeitenHMR TemplatepharmacisticusNoch keine Bewertungen
- Waqas Rahman CVDokument1 SeiteWaqas Rahman CVSalim AsgharNoch keine Bewertungen
- Philippines Pharmaceutical Country ProfileDokument347 SeitenPhilippines Pharmaceutical Country Profilemrk_rlndNoch keine Bewertungen
- Pharmaceutical IndustryDokument139 SeitenPharmaceutical IndustryIrtiza NoorNoch keine Bewertungen
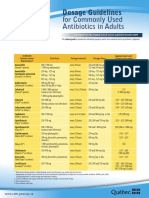
- CDM Antibio1 DosageGuidelines Adults enDokument2 SeitenCDM Antibio1 DosageGuidelines Adults endwiNoch keine Bewertungen
- Macrolides and LincosamidesDokument22 SeitenMacrolides and LincosamidesSunilNoch keine Bewertungen
- Bacopa MonnieriDokument5 SeitenBacopa MonnieriSanjeev GuptaNoch keine Bewertungen
- Process Safety and Environmental Protection: Baoyang DingDokument16 SeitenProcess Safety and Environmental Protection: Baoyang DingVipul BhagatNoch keine Bewertungen
- Cardiovascular Drugs and Medications Pharmacology QuizDokument7 SeitenCardiovascular Drugs and Medications Pharmacology QuizIsabel Bibat DavidNoch keine Bewertungen
- Harga Baru Ifars Juni 2022Dokument6 SeitenHarga Baru Ifars Juni 2022KeRtha NeghaRaNoch keine Bewertungen
- Chapter 48 - Drugs Affecting Blood CoagulationDokument12 SeitenChapter 48 - Drugs Affecting Blood CoagulationJonathon100% (1)
- Miacalcic NspyDokument9 SeitenMiacalcic NspyWagaJabalNoch keine Bewertungen
- Protein & Peptide Drug Delivery SystemDokument12 SeitenProtein & Peptide Drug Delivery SystemSandeep SainiNoch keine Bewertungen
- Pediatric PharmacotherapyDokument16 SeitenPediatric PharmacotherapyHamza Q. AhmedNoch keine Bewertungen
- Pharma Parenteral Dosage CalculationDokument3 SeitenPharma Parenteral Dosage CalculationMaxinne RoseñoNoch keine Bewertungen
- Test Bank For Basic Pharmacology For Nursing 17th EditionDokument10 SeitenTest Bank For Basic Pharmacology For Nursing 17th EditionUsman HaiderNoch keine Bewertungen
- Preparation and Evaluation of Solid Dispersion of Candesartan CilexetilDokument5 SeitenPreparation and Evaluation of Solid Dispersion of Candesartan CilexetilDeepu NaniNoch keine Bewertungen
- TobramycinSolution3msds PDFDokument6 SeitenTobramycinSolution3msds PDFMostofa RubalNoch keine Bewertungen
- Opioid Comparison Chart Prescriber Letter 2012 PDFDokument7 SeitenOpioid Comparison Chart Prescriber Letter 2012 PDFsrasrk11Noch keine Bewertungen
- Code of Ethics For Pharmacist - 1st Edition (June 2015)Dokument8 SeitenCode of Ethics For Pharmacist - 1st Edition (June 2015)Rhiza D. StrongholdNoch keine Bewertungen
- FIP Education Initiatives: Pharmacy Education Taskforce A Global Competency FrameworkDokument13 SeitenFIP Education Initiatives: Pharmacy Education Taskforce A Global Competency FrameworkLailaturrahmi LailaturrahmiNoch keine Bewertungen
- Dosage Calculation Review BookletDokument32 SeitenDosage Calculation Review BookletPatrick Eng100% (3)
- Adverse Drug Reactions: Key PointsDokument6 SeitenAdverse Drug Reactions: Key PointsOvi RifaniNoch keine Bewertungen
- Porter's Five Forces Analysis of Pharma SectorDokument3 SeitenPorter's Five Forces Analysis of Pharma SectorSakshi Goel100% (1)