Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Budget Plan Wound ClinicDokument4 SeitenBudget Plan Wound ClinicRegalado Aguhayon100% (1)
- Colour Atlas of Ophthalmic Plastic Surgery 4thDokument541 SeitenColour Atlas of Ophthalmic Plastic Surgery 4thsun seal100% (1)
- Operative ObstetricsDokument4 SeitenOperative Obstetricssarguss14100% (3)
- Sebaceous Hyperplasia Treatment With Combination oDokument2 SeitenSebaceous Hyperplasia Treatment With Combination oAndreNoch keine Bewertungen
- R Series Operator's Guide: 9650-0912-01 Rev. VDokument178 SeitenR Series Operator's Guide: 9650-0912-01 Rev. VA. A.G.Noch keine Bewertungen
- 0000 NFPA Gas System SizingDokument10 Seiten0000 NFPA Gas System SizingJohn ANoch keine Bewertungen
- JCM 10 02346Dokument16 SeitenJCM 10 02346Sergio Sitta TarquiniNoch keine Bewertungen
- Assisting The Patient During The Lumbar Puncture DefinitionDokument3 SeitenAssisting The Patient During The Lumbar Puncture DefinitionSHAINA CADALINNoch keine Bewertungen
- Grade 9: ScienceDokument19 SeitenGrade 9: ScienceChristian ArcegaNoch keine Bewertungen
- Abd 1Dokument33 SeitenAbd 1مريم مهندNoch keine Bewertungen
- Laryngofissure TechniqueDokument5 SeitenLaryngofissure TechniqueJamesNoch keine Bewertungen
- ACI CPG Care Adult Patients Acute TracheostomyDokument66 SeitenACI CPG Care Adult Patients Acute TracheostomyTùng KimNoch keine Bewertungen
- Nur 146 RleDokument47 SeitenNur 146 RleKeziah Marie Chua Santa-AnaNoch keine Bewertungen
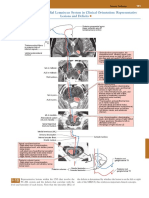
- Posterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsDokument1 SeitePosterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsEduardo RodriguezNoch keine Bewertungen
- National NORCET-3 - FinalDokument90 SeitenNational NORCET-3 - FinalSHIVANIINoch keine Bewertungen
- Mechanical Circulatory Support & Cardiothoracic Transplant: Friday 27 November 2020 Harefield HospitalDokument1 SeiteMechanical Circulatory Support & Cardiothoracic Transplant: Friday 27 November 2020 Harefield HospitalscudchssNoch keine Bewertungen
- Atlas of Orthopedic Surgical Procedures of The Dog and CatDokument244 SeitenAtlas of Orthopedic Surgical Procedures of The Dog and Catשאול רייס100% (4)
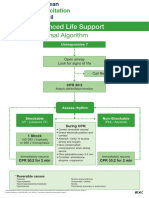
- Advanced Life Support - A0 PDFDokument1 SeiteAdvanced Life Support - A0 PDFiulia-uroNoch keine Bewertungen
- Physiology of One Lung Ventilation: Moderator-Dr. Nataraj Guide - Dr. Nagaraj Speaker - Dr. RohitDokument59 SeitenPhysiology of One Lung Ventilation: Moderator-Dr. Nataraj Guide - Dr. Nagaraj Speaker - Dr. RohitPraveen RamasamyNoch keine Bewertungen
- Session 2Dokument5 SeitenSession 2Sistine Rose LabajoNoch keine Bewertungen
- Mid FastDokument30 SeitenMid FastsujitmandotNoch keine Bewertungen
- Abdomen CAP Questions and AnswersDokument6 SeitenAbdomen CAP Questions and AnswersRathnaNoch keine Bewertungen
- Facial Danger ZonesDokument29 SeitenFacial Danger ZonesShamad AbduNoch keine Bewertungen
- What 'S New in Adult Reconstructive Knee Surgery: Guest EditorialDokument9 SeitenWhat 'S New in Adult Reconstructive Knee Surgery: Guest Editoriallllolll lllooollNoch keine Bewertungen
- WHO Surgical Safety ChecklistDokument1 SeiteWHO Surgical Safety ChecklistneculavNoch keine Bewertungen
- Angina Contemporary Diagnosis and ManagementDokument12 SeitenAngina Contemporary Diagnosis and Managementalejandro montesNoch keine Bewertungen
- Gastrointestinal System DisordersDokument112 SeitenGastrointestinal System DisordersTaate MohammedNoch keine Bewertungen
- Medical Terminolgy Trans 1 115 SlidesDokument14 SeitenMedical Terminolgy Trans 1 115 SlidesSophia Nicole LibaoNoch keine Bewertungen
- 11-C1 BrowliftDokument34 Seiten11-C1 BrowliftShaun Tan100% (1)
- Introduction To NeuroanatomyDokument20 SeitenIntroduction To NeuroanatomySurjagnee SannyamatNoch keine Bewertungen