Das könnte Ihnen auch gefallen
- Poetry Fest Room 5Dokument1 SeitePoetry Fest Room 5KatjVLNoch keine Bewertungen
- Room 5 Update: Dates To RememberDokument3 SeitenRoom 5 Update: Dates To RememberKatjVLNoch keine Bewertungen
- Selective Summarizer: Ame A e oDokument5 SeitenSelective Summarizer: Ame A e oKatjVLNoch keine Bewertungen
- Scan Doc0132Dokument8 SeitenScan Doc0132KatjVLNoch keine Bewertungen
- Scan Doc0103Dokument2 SeitenScan Doc0103KatjVLNoch keine Bewertungen
- Room 5 Update: Dates To RememberDokument3 SeitenRoom 5 Update: Dates To RememberKatjVLNoch keine Bewertungen
- Lit Circles For WEBSITEDokument10 SeitenLit Circles For WEBSITEKatjVLNoch keine Bewertungen
- Playground ProblemDokument4 SeitenPlayground ProblemKatjVLNoch keine Bewertungen
- Lit Circles For WEBSITEDokument10 SeitenLit Circles For WEBSITEKatjVLNoch keine Bewertungen
- Lit Circles For WEBSITEDokument10 SeitenLit Circles For WEBSITEKatjVLNoch keine Bewertungen
- Medical InvestigationDokument3 SeitenMedical InvestigationKatjVLNoch keine Bewertungen
- February 2010: Volunteer Schedule Room 5Dokument10 SeitenFebruary 2010: Volunteer Schedule Room 5KatjVLNoch keine Bewertungen
- Parent Conference ScheduleDokument2 SeitenParent Conference ScheduleKatjVLNoch keine Bewertungen
- December Problem SolvingDokument4 SeitenDecember Problem SolvingKatjVLNoch keine Bewertungen
- Mission ReportDokument6 SeitenMission ReportKatjVLNoch keine Bewertungen
- Scan Doc0066Dokument3 SeitenScan Doc0066KatjVLNoch keine Bewertungen
- Volunteer CalendarDokument6 SeitenVolunteer CalendarKatjVLNoch keine Bewertungen
- Parent Conference WeekDokument1 SeiteParent Conference WeekKatjVLNoch keine Bewertungen
- November 5Dokument2 SeitenNovember 5KatjVLNoch keine Bewertungen
- Room 5 CalendarDokument7 SeitenRoom 5 CalendarKatjVLNoch keine Bewertungen
- Scholastic Book Order (Parent Letter)Dokument1 SeiteScholastic Book Order (Parent Letter)KatjVLNoch keine Bewertungen
- Volunteer CalendarDokument7 SeitenVolunteer CalendarKatjVLNoch keine Bewertungen
- Volunteer CalendarDokument8 SeitenVolunteer CalendarKatjVLNoch keine Bewertungen
- Room 5 CalendarDokument9 SeitenRoom 5 CalendarKatjVLNoch keine Bewertungen
- Room 5 CalendarDokument8 SeitenRoom 5 CalendarKatjVLNoch keine Bewertungen
- Scan Doc0066Dokument3 SeitenScan Doc0066KatjVLNoch keine Bewertungen
- I? BPL M - Iving: Roup Gtpo. 1E Fkmthi.) IDokument4 SeitenI? BPL M - Iving: Roup Gtpo. 1E Fkmthi.) IKatjVLNoch keine Bewertungen
- Scan Doc0066Dokument3 SeitenScan Doc0066KatjVLNoch keine Bewertungen
- Election PacketDokument8 SeitenElection PacketKatjVLNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Emp Master 09042015Dokument80 SeitenEmp Master 09042015Joe SalisNoch keine Bewertungen
- Asanthe Case WorkingsDokument9 SeitenAsanthe Case Workingsazhar hussainNoch keine Bewertungen
- RubyDokument13 SeitenRubyNamoAmitofouNoch keine Bewertungen
- The Significance of Immunization in The Prevention of Childhood Killer DiseasesDokument69 SeitenThe Significance of Immunization in The Prevention of Childhood Killer DiseasesUsman Ahmad TijjaniNoch keine Bewertungen
- Case Study Clinical Application of Nightingale - S Environmental TheoryDokument5 SeitenCase Study Clinical Application of Nightingale - S Environmental TheorysannsannNoch keine Bewertungen
- Provisional Rank List for MBBS/BDS 2020-2021 Management QuotaDokument476 SeitenProvisional Rank List for MBBS/BDS 2020-2021 Management QuotaDfhjjNoch keine Bewertungen
- Comparison of Services Between Public and Private HospitalsDokument10 SeitenComparison of Services Between Public and Private HospitalsJahidul IslamNoch keine Bewertungen
- MS Case # 4 - Endo, Uro, Burns, FE & AB ImbalancDokument3 SeitenMS Case # 4 - Endo, Uro, Burns, FE & AB ImbalancDemocrito Louierick Plaza VINoch keine Bewertungen
- MPT Musculoskeletal Physiotherapy-Smt Kashibai Navale College of Physiotherapy, Pune - Admission-Details - 20230925204502Dokument3 SeitenMPT Musculoskeletal Physiotherapy-Smt Kashibai Navale College of Physiotherapy, Pune - Admission-Details - 20230925204502hindjai66Noch keine Bewertungen
- Dip PEC (SA) Past Papers - 2011 Sept 29 1 2014Dokument5 SeitenDip PEC (SA) Past Papers - 2011 Sept 29 1 2014matentenNoch keine Bewertungen
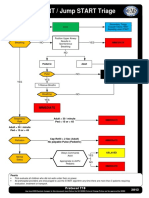
- Start - Jump START Triage PDFDokument2 SeitenStart - Jump START Triage PDF081381246529100% (1)
- Myasthenia Gravis With Respiratory Failure in The Intensive Care UnitDokument4 SeitenMyasthenia Gravis With Respiratory Failure in The Intensive Care UnitDr. FarhanNoch keine Bewertungen
- Encephalopathy HepaticumDokument2 SeitenEncephalopathy Hepaticumtitis dwi tantiNoch keine Bewertungen
- CPH WEEK 3: EPIDEMIOLOGY (PART 1Dokument1 SeiteCPH WEEK 3: EPIDEMIOLOGY (PART 1Shane G.Noch keine Bewertungen
- Laboratory No. 1 Introduction To Human Body Scope of Laboratory ActivityDokument6 SeitenLaboratory No. 1 Introduction To Human Body Scope of Laboratory ActivityOSHIEN PENELOPE ABADIANoch keine Bewertungen
- Presentasi Produk HDPIDokument62 SeitenPresentasi Produk HDPIBoy Royen Vikri NababanNoch keine Bewertungen
- Contingency PLAN COVID 19 FIN Sept 29 2022Dokument35 SeitenContingency PLAN COVID 19 FIN Sept 29 2022Fabro F. MhiseyNoch keine Bewertungen
- Quality Assurance ProgramDokument16 SeitenQuality Assurance ProgramMyca Omega Lacsamana100% (1)
- Reading Daily ActivitiesDokument3 SeitenReading Daily ActivitiesHafid JuniorNoch keine Bewertungen
- Professional Issues in Clinical PsychologyDokument5 SeitenProfessional Issues in Clinical PsychologyJohn Moone100% (2)
- Mental Health Nursing GuideDokument32 SeitenMental Health Nursing GuideMegha V Kurian60% (5)
- Jurnal Amik SanglahDokument6 SeitenJurnal Amik Sanglahslamet pujianto SkepNoch keine Bewertungen
- Acing The Orthopedic Board ExamDokument481 SeitenAcing The Orthopedic Board ExamMark M. Alipio100% (9)
- Acrylic Partial Dentures More Satisfying Than Cast DenturesDokument4 SeitenAcrylic Partial Dentures More Satisfying Than Cast DenturesAkikoz N SevenNoch keine Bewertungen
- Infection Control in NICUDokument9 SeitenInfection Control in NICUMike CalipayanNoch keine Bewertungen
- Annotated Bibliograhy: Submitted ToDokument4 SeitenAnnotated Bibliograhy: Submitted ToRumela Ganguly ChakrabortyNoch keine Bewertungen
- Dentistry Associate Cover Letter 1Dokument2 SeitenDentistry Associate Cover Letter 1nicoleclchuaNoch keine Bewertungen
- Bills Approved or Enacted by Gov. McAuliffeDokument13 SeitenBills Approved or Enacted by Gov. McAuliffeWSETNoch keine Bewertungen
- 50 Big Debates in Gynecologic Oncology (2023) - Dennis S. ChiDokument351 Seiten50 Big Debates in Gynecologic Oncology (2023) - Dennis S. ChiGardener Ayu100% (1)
- SIP ReportDokument65 SeitenSIP ReportLUCKY NAZARNoch keine Bewertungen