Das könnte Ihnen auch gefallen
- Rocabado Pain Map For Evaluating TMDDokument11 SeitenRocabado Pain Map For Evaluating TMDNeagu EmaNoch keine Bewertungen
- InTech-Molar Incisor Hypomineralization Morphological Aetiological Epidemiological and Clinical ConsiderationsDokument25 SeitenInTech-Molar Incisor Hypomineralization Morphological Aetiological Epidemiological and Clinical ConsiderationsNeagu EmaNoch keine Bewertungen
- Intergeneric Communication in Dental Plaque Biofilms: Expression of Fima Is Regulated by S. CristatusDokument4 SeitenIntergeneric Communication in Dental Plaque Biofilms: Expression of Fima Is Regulated by S. CristatusNeagu EmaNoch keine Bewertungen
- 6.Nield-Gehrig, J. S. Dental Plaque Biofilms. Dental Plaque Biofilms. Marsh, P.D. Dental Plaque as a Biofilm and a Microbial Community - Implications for Health and Disease. BMC Oral Health. 2006. 6 (Suppl 1)Dokument8 Seiten6.Nield-Gehrig, J. S. Dental Plaque Biofilms. Dental Plaque Biofilms. Marsh, P.D. Dental Plaque as a Biofilm and a Microbial Community - Implications for Health and Disease. BMC Oral Health. 2006. 6 (Suppl 1)Neagu EmaNoch keine Bewertungen
- Oral Health Status of Children and Adults in Urban and Rural Areas of Burkina Faso, AfricaDokument7 SeitenOral Health Status of Children and Adults in Urban and Rural Areas of Burkina Faso, AfricaNeagu EmaNoch keine Bewertungen
- Oral Health ChineseDokument9 SeitenOral Health ChineseNeagu EmaNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Ee-502 Unit - IDokument2 SeitenEe-502 Unit - IVARAPRASADNoch keine Bewertungen
- Mod 4 Revision Guide 1 Reaction Kinetics AQA A2 ChemistryDokument5 SeitenMod 4 Revision Guide 1 Reaction Kinetics AQA A2 Chemistryviyas07Noch keine Bewertungen
- SpiralDokument47 SeitenSpiralEr. Vicky MakawanaNoch keine Bewertungen
- Pelod Vs Sofa Scoring in PediatricDokument6 SeitenPelod Vs Sofa Scoring in PediatricAdrian KhomanNoch keine Bewertungen
- Comptector & Chiller (Cdu) Controller (Fx32C Series) : Precaution For UseDokument5 SeitenComptector & Chiller (Cdu) Controller (Fx32C Series) : Precaution For UseFcma0903100% (1)
- Real Time Operating SystemsDokument15 SeitenReal Time Operating SystemsSaro VrsNoch keine Bewertungen
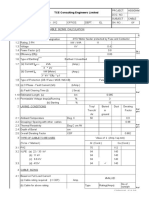
- Cable Sizing CalculationDokument72 SeitenCable Sizing CalculationHARI my songs100% (1)
- Case StudyDokument10 SeitenCase StudyVintage ArtNoch keine Bewertungen
- CISCO Router Software - Configuration PDFDokument408 SeitenCISCO Router Software - Configuration PDFasalihovicNoch keine Bewertungen
- An FPGA Implementation of A Feed-Back Chaotic Synchronization For Secure CommunicationsDokument5 SeitenAn FPGA Implementation of A Feed-Back Chaotic Synchronization For Secure Communicationslaz_chikhi1574Noch keine Bewertungen
- Spelling RulesDokument5 SeitenSpelling RulesvijthorNoch keine Bewertungen
- Tecumseh Parts List OHV 135Dokument5 SeitenTecumseh Parts List OHV 135M MNoch keine Bewertungen
- V1 N2 1980 RabenhorstDokument6 SeitenV1 N2 1980 Rabenhorstraa2010Noch keine Bewertungen
- Ss 1 Further Mathematics Lesson 4Dokument7 SeitenSs 1 Further Mathematics Lesson 4Adio Babatunde Abiodun CabaxNoch keine Bewertungen
- FP 3000 PDFDokument1 SeiteFP 3000 PDFClaudio Godoy ZepedaNoch keine Bewertungen
- FST 3000Dokument4 SeitenFST 3000ariksyaiful82Noch keine Bewertungen
- Auto-Tune Pid Temperature & Timer General Specifications: N L1 L2 L3Dokument4 SeitenAuto-Tune Pid Temperature & Timer General Specifications: N L1 L2 L3sharawany 20Noch keine Bewertungen
- 1922 A Textbook of Balochi LanguageDokument228 Seiten1922 A Textbook of Balochi LanguageAnonymous 0ywnNS29EGNoch keine Bewertungen
- 100 TOP Real Time Objective C Multiple Choice Questions and Answers PDF DownloadDokument22 Seiten100 TOP Real Time Objective C Multiple Choice Questions and Answers PDF DownloadNayan BariNoch keine Bewertungen
- 2D Pipeline Bottom Roughness - Mochammad ImronDokument6 Seiten2D Pipeline Bottom Roughness - Mochammad ImronLK AnhDungNoch keine Bewertungen
- Jazz Piano VoicingsDokument19 SeitenJazz Piano Voicingskeybiank86% (58)
- Bobrick 2021 Class. Quantum Grav. 38 105009Dokument23 SeitenBobrick 2021 Class. Quantum Grav. 38 105009MaxNoch keine Bewertungen
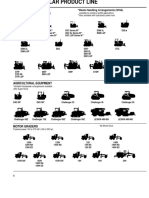
- Caterpillar Product Line 13Dokument7 SeitenCaterpillar Product Line 13GenneraalNoch keine Bewertungen
- Knowage Suite Readthedocs Io en 7.4Dokument536 SeitenKnowage Suite Readthedocs Io en 7.4Sergio Daniel Marambio NuñezNoch keine Bewertungen
- Comparative Study of Steel Structure With and Without Floating Columns in EtabsDokument13 SeitenComparative Study of Steel Structure With and Without Floating Columns in EtabsBehroz BehzadNoch keine Bewertungen
- AtomDokument15 SeitenAtomdewi murtasimaNoch keine Bewertungen
- 03 ModularizationDokument5 Seiten03 ModularizationsumnatarajNoch keine Bewertungen
- Ball Charge ManagementDokument14 SeitenBall Charge ManagementSalud Y SucesosNoch keine Bewertungen
- Leading The Industry In: Solar Microinverter TechnologyDokument2 SeitenLeading The Industry In: Solar Microinverter TechnologydukegaloNoch keine Bewertungen
- Good 1983Dokument352 SeitenGood 1983ASDA75% (4)