Das könnte Ihnen auch gefallen
- Cardiovascular MneumonicsDokument10 SeitenCardiovascular MneumonicsKaly RieNoch keine Bewertungen
- ACLS Manual Provider 2016Dokument207 SeitenACLS Manual Provider 2016AhmedShareef100% (9)
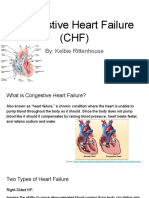
- CHFDokument61 SeitenCHFAngeline Lareza-Reyna VillasorNoch keine Bewertungen
- The Amazing Way to Reverse Heart Disease Naturally: Beyond the Hypertension Hype: Why Drugs Are Not the AnswerVon EverandThe Amazing Way to Reverse Heart Disease Naturally: Beyond the Hypertension Hype: Why Drugs Are Not the AnswerBewertung: 5 von 5 Sternen5/5 (2)
- Cardiac Stress TestingDokument90 SeitenCardiac Stress TestingFrancesca Isabel BunyiNoch keine Bewertungen
- CardiologyDokument345 SeitenCardiologyClaudiu Ungureanu Clau100% (3)
- EKGDokument137 SeitenEKGGbariel100% (3)
- Diabetes Control-How to Lower Blood Pressure NaturallyVon EverandDiabetes Control-How to Lower Blood Pressure NaturallyBewertung: 5 von 5 Sternen5/5 (1)
- Defibrillation and CardioversionDokument40 SeitenDefibrillation and CardioversionKusum Roy100% (1)
- Basic ECG Lecture - NewDokument148 SeitenBasic ECG Lecture - NewAradhanaRamchandaniNoch keine Bewertungen
- Hypertension: A Neglecting IllnessDokument15 SeitenHypertension: A Neglecting IllnessKaren GonzalesNoch keine Bewertungen
- INTERNAL MEDICINE - Cardiovascular SystemDokument8 SeitenINTERNAL MEDICINE - Cardiovascular SystemAiswaryaNoch keine Bewertungen
- User's Guide to Policosanol & Other Natural Ways to Lower Cholesterol: Learn about the Many Safe Ways to Reduce Your Cholesterol and Lower Your Risk of Heart DiseaseVon EverandUser's Guide to Policosanol & Other Natural Ways to Lower Cholesterol: Learn about the Many Safe Ways to Reduce Your Cholesterol and Lower Your Risk of Heart DiseaseNoch keine Bewertungen
- 991111 EUS教學 (6) 重點式急診心臟超音波之應用Dokument67 Seiten991111 EUS教學 (6) 重點式急診心臟超音波之應用juice119100% (5)
- Activity 11 Cardiac Tamponade NCPDokument3 SeitenActivity 11 Cardiac Tamponade NCPCloe CorpuzNoch keine Bewertungen
- (The European Society of Cardiology Series) Marco Tubaro (Editor), Pascal Vranckx (Editor), Susanna Price (Editor), Christiaan Vrints (Editor), Eric Bonnefoy (Editor) - The ESC Textbook of Intensive ADokument1.088 Seiten(The European Society of Cardiology Series) Marco Tubaro (Editor), Pascal Vranckx (Editor), Susanna Price (Editor), Christiaan Vrints (Editor), Eric Bonnefoy (Editor) - The ESC Textbook of Intensive AEdu MartinsNoch keine Bewertungen
- Coronary Heart DiseaseDokument13 SeitenCoronary Heart DiseaseLea Recto VinuyaNoch keine Bewertungen
- Disease Presentation: HypertensionDokument9 SeitenDisease Presentation: HypertensionAprilyn Magsigay100% (1)
- Hypertension & Stroke: Prepared By: Sharinah Ainee S. Pasandalan BSN-III, Group 4Dokument56 SeitenHypertension & Stroke: Prepared By: Sharinah Ainee S. Pasandalan BSN-III, Group 4Sharinah Ainee Sabalburo PasandalanNoch keine Bewertungen
- PBL 1 HypertensionDokument11 SeitenPBL 1 HypertensionLaughin KowNoch keine Bewertungen
- Heart Disease in The Elderly: Lawrence H. Young, M.DDokument9 SeitenHeart Disease in The Elderly: Lawrence H. Young, M.DBurghelea Ovidiu-GabrielNoch keine Bewertungen
- Congestive Heart Failure FinalxxxxDokument12 SeitenCongestive Heart Failure FinalxxxxDoneva Lyn MedinaNoch keine Bewertungen
- Early Warning Signs Your Blood Pressure Is Dangerously HighDokument9 SeitenEarly Warning Signs Your Blood Pressure Is Dangerously HighRatnaPrasadNalamNoch keine Bewertungen
- What Is Cardiovascular Disease?Dokument6 SeitenWhat Is Cardiovascular Disease?Logeshwaran ArunNoch keine Bewertungen
- Heart Attack Risk Factors: Non-Coronary Artery Disease Causes of Heart Attack May Also Occur, These IncludeDokument12 SeitenHeart Attack Risk Factors: Non-Coronary Artery Disease Causes of Heart Attack May Also Occur, These IncludeHazwan AkmalNoch keine Bewertungen
- What Is Hypertension? What Causes Hypertension?Dokument5 SeitenWhat Is Hypertension? What Causes Hypertension?Walaako MaisipNoch keine Bewertungen
- Fadhilah (Hearth Desease)Dokument4 SeitenFadhilah (Hearth Desease)Fadhilah DhilahNoch keine Bewertungen
- MT23 3rd CHFDokument6 SeitenMT23 3rd CHFKenneth OliverNoch keine Bewertungen
- Understanding Systolic Hypertension in The Elderly: R Gupta, RR KasliwalDokument7 SeitenUnderstanding Systolic Hypertension in The Elderly: R Gupta, RR KasliwallolitlolatNoch keine Bewertungen
- Arterial ThrombosisDokument4 SeitenArterial ThrombosisFaraida Jilzani ArsadNoch keine Bewertungen
- Overview (Intro - Clinical Manifestations, Causes, Risk Factors, Complications, Prevention) Assessment, Diagnosis (Med and Nursing)Dokument27 SeitenOverview (Intro - Clinical Manifestations, Causes, Risk Factors, Complications, Prevention) Assessment, Diagnosis (Med and Nursing)Luayon FrancisNoch keine Bewertungen
- Heart Attack (Myocardial Infarction)Dokument4 SeitenHeart Attack (Myocardial Infarction)Mack Javier VenturaNoch keine Bewertungen
- Chapter 13 CirculationDokument27 SeitenChapter 13 CirculationHerman ZoletaNoch keine Bewertungen
- This Is ItDokument6 SeitenThis Is Itjagipeb439Noch keine Bewertungen
- Medications Various Drugs Can Slow - or Even Reverse - The Effects of Atherosclerosis. Here AreDokument8 SeitenMedications Various Drugs Can Slow - or Even Reverse - The Effects of Atherosclerosis. Here Areluis fernando santos narvaezNoch keine Bewertungen
- PHN Assign 2Dokument13 SeitenPHN Assign 2ghulam anooshaNoch keine Bewertungen
- BIOLOGY PROJECT (Class 12)Dokument21 SeitenBIOLOGY PROJECT (Class 12)Manoghna MaheshNoch keine Bewertungen
- Case Study For Coronary Artery DiseaseDokument8 SeitenCase Study For Coronary Artery DiseaseGabbii CincoNoch keine Bewertungen
- Hypertension IDokument14 SeitenHypertension IHilary PasiliaoNoch keine Bewertungen
- Hypertension and The Cardiac DietDokument3 SeitenHypertension and The Cardiac DietKate MckinneyNoch keine Bewertungen
- Hypertension - OkeDokument4 SeitenHypertension - OkeKhaleda FatmawatiNoch keine Bewertungen
- Heart Disease DissertationDokument6 SeitenHeart Disease DissertationWriteMyPaperForMeIn3HoursMilwaukee100% (1)
- Cardio DiseaseDokument12 SeitenCardio DiseaseEsnaira EbrahimNoch keine Bewertungen
- Causes Symptoms Diagnosis and TreatmentDokument10 SeitenCauses Symptoms Diagnosis and TreatmentcellinectnNoch keine Bewertungen
- Report About HypertensionDokument11 SeitenReport About HypertensionZA IDNoch keine Bewertungen
- Management of Common Medical Problems of the Elderly in Plain (Non-Medical) LanguageVon EverandManagement of Common Medical Problems of the Elderly in Plain (Non-Medical) LanguageNoch keine Bewertungen
- Hypertensive Cardiovascular Disease Also Known As Hypertensive Heart Disease Occurs Due To The Complication of Hypertension or High Blood PressureDokument3 SeitenHypertensive Cardiovascular Disease Also Known As Hypertensive Heart Disease Occurs Due To The Complication of Hypertension or High Blood Pressurejoanneceline16Noch keine Bewertungen
- Hypertension: Jumarang, Kim Enrico M. BSN401 STI - Global CityDokument6 SeitenHypertension: Jumarang, Kim Enrico M. BSN401 STI - Global CityKim Enrico JumarangNoch keine Bewertungen
- PPISMP SEM 2 BIOLOGY Cardiovascular DiseaseDokument5 SeitenPPISMP SEM 2 BIOLOGY Cardiovascular DiseaseMohamad Syafie Bin SamsirNoch keine Bewertungen
- Written Report Coronary Heart DiseaseDokument5 SeitenWritten Report Coronary Heart DiseaseJade WushuNoch keine Bewertungen
- Q&As On HypertensionDokument5 SeitenQ&As On HypertensionLynda Asita SharaNoch keine Bewertungen
- Cardiovascular DiseaseDokument7 SeitenCardiovascular DiseaseCharlenaNoch keine Bewertungen
- Some Medical Questions and AnswersDokument12 SeitenSome Medical Questions and AnswersShereen AlobinayNoch keine Bewertungen
- Cardiovascular DiseaseDokument9 SeitenCardiovascular Diseaseiri_balNoch keine Bewertungen
- Hypertension and Congestive Heart FailureDokument4 SeitenHypertension and Congestive Heart FailureDawn ReyaNoch keine Bewertungen
- Heart Failure and CKD: What You Need To KnowDokument2 SeitenHeart Failure and CKD: What You Need To KnowHarsh0% (1)
- Pe 1 Lesson 2 Non-Communicable DiseasesDokument79 SeitenPe 1 Lesson 2 Non-Communicable Diseasesdario serranoNoch keine Bewertungen
- HF Congestive Heart Failure 2Dokument3 SeitenHF Congestive Heart Failure 2Yuppie RajNoch keine Bewertungen
- BioDokument32 SeitenBioPriyanka RNoch keine Bewertungen
- Bhs Inggrs TransletDokument6 SeitenBhs Inggrs TransletArif AshariNoch keine Bewertungen
- Hipertension en El AncianoDokument11 SeitenHipertension en El AncianoEdgar G RoblesNoch keine Bewertungen
- ReportDokument28 SeitenReportHazel KingNoch keine Bewertungen
- Congestive Heart Failure CHFDokument13 SeitenCongestive Heart Failure CHFapi-674402238Noch keine Bewertungen
- Heart Diseases Are Indeed TheDokument4 SeitenHeart Diseases Are Indeed TheHANNAH TOH HONG NA MoeNoch keine Bewertungen
- X-Plain Essential Hypertension: Reference SummaryDokument0 SeitenX-Plain Essential Hypertension: Reference Summaryrys239Noch keine Bewertungen
- Science Folio FINALESTDokument13 SeitenScience Folio FINALESTDesNoch keine Bewertungen
- HypertensionDokument3 SeitenHypertensionLeirish PabionNoch keine Bewertungen
- AssignmentDokument4 SeitenAssignmentDáńí KħâŋNoch keine Bewertungen
- Exercise Prescription & ProgrammingDokument34 SeitenExercise Prescription & ProgrammingSmiley Jhen Garcia SabinianoNoch keine Bewertungen
- Acs Nstemi Ua PathoDokument9 SeitenAcs Nstemi Ua PathoClaring CiprianoNoch keine Bewertungen
- Paediatric CardiologyDokument15 SeitenPaediatric CardiologyAaron Nameer Abrar RahmanNoch keine Bewertungen
- The Diagnosis and Treatment of Pulmonary Valve SteDokument6 SeitenThe Diagnosis and Treatment of Pulmonary Valve SteNiarti Ulan SariNoch keine Bewertungen
- Case Report: Probable Case of Infective EndocarditisDokument5 SeitenCase Report: Probable Case of Infective EndocarditisJuan Jose SanchezNoch keine Bewertungen
- Ecg ReadingDokument2 SeitenEcg Readingtheodore_estradaNoch keine Bewertungen
- Pha CPR Bls Acls Manual 2012 Edited (08 25 2012)Dokument30 SeitenPha CPR Bls Acls Manual 2012 Edited (08 25 2012)Gene Alfonso BanawaNoch keine Bewertungen
- Ibutilide FumarateDokument3 SeitenIbutilide Fumarateapi-3797941Noch keine Bewertungen
- Clinical Practice GuidelinesDokument9 SeitenClinical Practice GuidelinesIntel AtomNoch keine Bewertungen
- I. Skenario A: 2. Muffle Heart SoundsDokument6 SeitenI. Skenario A: 2. Muffle Heart SoundsJefri SoniNoch keine Bewertungen
- Preoperative Cardiac Risk Assessment in Noncardiac SurgeryDokument6 SeitenPreoperative Cardiac Risk Assessment in Noncardiac SurgeryOgbonnaya IfeanyichukwuNoch keine Bewertungen
- Full Programme 9Dokument18 SeitenFull Programme 9Borneo CTVSNoch keine Bewertungen
- Pharmacology of Disopyramide: Yosephine A. H. 020100058Dokument20 SeitenPharmacology of Disopyramide: Yosephine A. H. 020100058zulfantri1983Noch keine Bewertungen
- Cardiac QuestionsDokument13 SeitenCardiac Questionsacque100% (1)
- Sono 338 - Echocardiography-Worksheet 2017Dokument2 SeitenSono 338 - Echocardiography-Worksheet 2017api-347648847Noch keine Bewertungen
- Aed Medical Abbreviation - Google SearchDokument1 SeiteAed Medical Abbreviation - Google SearchDanlexNoch keine Bewertungen
- Career Paths Nursing SBDokument12 SeitenCareer Paths Nursing SBAy ManNoch keine Bewertungen
- Truncus Arteriosu1Dokument3 SeitenTruncus Arteriosu1Zem KhazzyNoch keine Bewertungen
- Scholarly Sources Annotated Bibliography 1Dokument14 SeitenScholarly Sources Annotated Bibliography 1api-585127618Noch keine Bewertungen
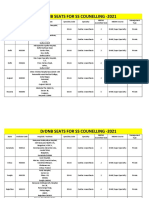
- Final DRDNB Seats For SS Counselling 2021Dokument152 SeitenFinal DRDNB Seats For SS Counselling 2021Pavan KumarNoch keine Bewertungen
- Physiology of The HeartDokument27 SeitenPhysiology of The HeartNavadeep KalluriNoch keine Bewertungen