Das könnte Ihnen auch gefallen
- Methodologies for Seismic Safety Evaluation of Existing Nuclear InstallationsVon EverandMethodologies for Seismic Safety Evaluation of Existing Nuclear InstallationsNoch keine Bewertungen
- IJIE 07 211 R1 EdDokument39 SeitenIJIE 07 211 R1 EdAnand sharmaNoch keine Bewertungen
- Fatigue Assessment in Light Water Reactors for Long Term Operation: Good Practices and Lessons LearnedVon EverandFatigue Assessment in Light Water Reactors for Long Term Operation: Good Practices and Lessons LearnedNoch keine Bewertungen
- RR 766Dokument126 SeitenRR 766Anand sharmaNoch keine Bewertungen
- Hydraulic Rock BreakerDokument10 SeitenHydraulic Rock BreakerMarcos NoronhaNoch keine Bewertungen
- Ibrahim 2020 IOP Conf. Ser. Mater. Sci. Eng. 834 012056 PDFDokument7 SeitenIbrahim 2020 IOP Conf. Ser. Mater. Sci. Eng. 834 012056 PDFerlangga naurianNoch keine Bewertungen
- Application of Probabilistic Methods for the Safety Assessment and the Reliable Operation of Research ReactorsVon EverandApplication of Probabilistic Methods for the Safety Assessment and the Reliable Operation of Research ReactorsNoch keine Bewertungen
- Dynamic Optimization Design of Cranes Based On Human-Crane-Rail System Dynamics and Annoyance RateDokument19 SeitenDynamic Optimization Design of Cranes Based On Human-Crane-Rail System Dynamics and Annoyance RateGogyNoch keine Bewertungen
- ISO TC159 SC3 Standards - Annotated AbstractsDokument8 SeitenISO TC159 SC3 Standards - Annotated AbstractsHéctor Eduardo Hernández LópezNoch keine Bewertungen
- Plewa Et Al 2012 Comparison Between Iso 2631 1 Comfort Prediction Equations and Self Reported Comfort Values DuringDokument11 SeitenPlewa Et Al 2012 Comparison Between Iso 2631 1 Comfort Prediction Equations and Self Reported Comfort Values DuringHuang XiaodianNoch keine Bewertungen
- Occupational Vibration in Urban Bus and Influence On Driver's Lower Limbs: A ReviewDokument11 SeitenOccupational Vibration in Urban Bus and Influence On Driver's Lower Limbs: A ReviewMarko CvetkovićNoch keine Bewertungen
- Risk AssesmentDokument13 SeitenRisk AssesmentORIENT YOUR CAREERNoch keine Bewertungen
- Chen 2009Dokument11 SeitenChen 2009ZulkarnainNoch keine Bewertungen
- Rob Band Mansfield ArticleDokument30 SeitenRob Band Mansfield ArticleJhet CoritanaNoch keine Bewertungen
- Hazards Identification of Eot Cranes and Their Control MeasuresDokument8 SeitenHazards Identification of Eot Cranes and Their Control Measuressiddhu mendheNoch keine Bewertungen
- A Report Based On Analysis of Posture and OccupatiDokument8 SeitenA Report Based On Analysis of Posture and OccupatiJOSE JAVIER BARZALLO GALVEZNoch keine Bewertungen
- An Observational Method For Postural Ergonomic Risk Assessment (PERA)Dokument19 SeitenAn Observational Method For Postural Ergonomic Risk Assessment (PERA)ttorrespoNoch keine Bewertungen
- Trolleys - HSE, UKDokument105 SeitenTrolleys - HSE, UKNgaire Pettit-YoungNoch keine Bewertungen
- FEM Used in Improvement of Quality of Medical DeviDokument9 SeitenFEM Used in Improvement of Quality of Medical DeviAnonymous P8Bt46mk5INoch keine Bewertungen
- Measurement and Evaluation of Whole Body Vibrationexposure in Drivers of Cargo Vehicle CompositionsDokument12 SeitenMeasurement and Evaluation of Whole Body Vibrationexposure in Drivers of Cargo Vehicle CompositionsAnand sharmaNoch keine Bewertungen
- Whole Body Vibration Exposure and Its Effects On Heavy Earth Moving Machinery PDFDokument11 SeitenWhole Body Vibration Exposure and Its Effects On Heavy Earth Moving Machinery PDFAnandNoch keine Bewertungen
- The European Vibration Directive: Review ArticleDokument8 SeitenThe European Vibration Directive: Review ArticleAnand sharmaNoch keine Bewertungen
- Correcting Working Postures in Industry: A Practical Method For AnalysisDokument3 SeitenCorrecting Working Postures in Industry: A Practical Method For AnalysissubirNoch keine Bewertungen
- Musculoskeletal Disorder (MSD) Risk Assessment ToolsDokument15 SeitenMusculoskeletal Disorder (MSD) Risk Assessment ToolsJulio Alberto Pambabay SantacruzNoch keine Bewertungen
- Improving The Work Position of Worker's Based On Quick Exposure Check Method To Reduce The Risk of Work Related Musculoskeletal DisordersDokument8 SeitenImproving The Work Position of Worker's Based On Quick Exposure Check Method To Reduce The Risk of Work Related Musculoskeletal DisorderssauravNoch keine Bewertungen
- Iso 2631Dokument10 SeitenIso 2631Arsyadul EbaadNoch keine Bewertungen
- Vibration Exposure and Control: A Case Study With Practical AssessmentDokument11 SeitenVibration Exposure and Control: A Case Study With Practical AssessmentAnand sharmaNoch keine Bewertungen
- Griffin 1998Dokument32 SeitenGriffin 1998Pankaj SharmaNoch keine Bewertungen
- A Guide To: Whole-Body Vibration: January 2005Dokument33 SeitenA Guide To: Whole-Body Vibration: January 2005drnvkrishnaNoch keine Bewertungen
- A - Comparative - Study - of - Whole-Body - Vibration - ExposuDokument14 SeitenA - Comparative - Study - of - Whole-Body - Vibration - ExposuMuhd AfiqNoch keine Bewertungen
- Effect of Motor Vehicle Structural Vibration On Human Body - ReviewDokument5 SeitenEffect of Motor Vehicle Structural Vibration On Human Body - ReviewVignesh KumarNoch keine Bewertungen
- Health Effect of Whole Body VibrationDokument11 SeitenHealth Effect of Whole Body Vibrationsushirdj999100% (1)
- A Review On Ergonomic Risk Factors Causing Musculoskeletal Disorders Among Construction Workers IJERTV9IS060887Dokument3 SeitenA Review On Ergonomic Risk Factors Causing Musculoskeletal Disorders Among Construction Workers IJERTV9IS060887Jeisther Timothy GalanoNoch keine Bewertungen
- Iso 14243 1 2002 FR PDFDokument8 SeitenIso 14243 1 2002 FR PDFRobe01Noch keine Bewertungen
- HSE Hoop BucklingDokument153 SeitenHSE Hoop BucklingStokes21Noch keine Bewertungen
- Product Risk Management Report For Spine ProductsDokument25 SeitenProduct Risk Management Report For Spine ProductsAlejandro Landinez100% (1)
- 01 Wirtz GearTransmissionMonitoringDokument14 Seiten01 Wirtz GearTransmissionMonitoringdusan cincarNoch keine Bewertungen
- ITTC 75-02-05-041 Seasickness and FatigueDokument5 SeitenITTC 75-02-05-041 Seasickness and FatigueRamzi GuantengNoch keine Bewertungen
- ISO 21534 Non-Active SurgicalDokument8 SeitenISO 21534 Non-Active SurgicalDiego Sebastian Rojas GodoyNoch keine Bewertungen
- Fatigue Design FaDokument6 SeitenFatigue Design FaSani Adipura WinataNoch keine Bewertungen
- JAEHR - Volume 2 - Issue 2 - Pages 65-71Dokument7 SeitenJAEHR - Volume 2 - Issue 2 - Pages 65-71Shafiul AlamNoch keine Bewertungen
- On Field Tractor Seat Vibration AnalysisDokument7 SeitenOn Field Tractor Seat Vibration AnalysisjdamjanNoch keine Bewertungen
- HSE (Trainor Et Al) - 2006 - HSE Report No 426 ACUTEXDokument106 SeitenHSE (Trainor Et Al) - 2006 - HSE Report No 426 ACUTEXKhuda Buksh100% (1)
- 3dmotion BasedergonomicriskassessmentframeworkanditsvalidationmethodDokument32 Seiten3dmotion BasedergonomicriskassessmentframeworkanditsvalidationmethodSze ZhaoNoch keine Bewertungen
- Comparison of ISO 14243-1 To ASTM F3141 in Terms of Wearing of Knee Prostheses - ScienceDirectDokument19 SeitenComparison of ISO 14243-1 To ASTM F3141 in Terms of Wearing of Knee Prostheses - ScienceDirectEzgi PelitNoch keine Bewertungen
- Comparison Reba and QecDokument7 SeitenComparison Reba and Qecm_myfrenNoch keine Bewertungen
- 103Dokument9 Seiten103ieom2012Noch keine Bewertungen
- Ergonomic Evaluation To Improve Work Posture IJERTV5IS031136Dokument9 SeitenErgonomic Evaluation To Improve Work Posture IJERTV5IS031136NIRAJ NARSINGDAS BHATTADNoch keine Bewertungen
- OWAS (Ovako Working Posture Assessment System) : General Description and Development of The MethodDokument6 SeitenOWAS (Ovako Working Posture Assessment System) : General Description and Development of The Methodgeklan_Noch keine Bewertungen
- Whole Body VibrationDokument7 SeitenWhole Body Vibrationinsync_001Noch keine Bewertungen
- Agreement Between Observed and Interview - Based Exposure To Ergonomics Factors For The Upper Extremities in Employees of A Package Sorting PlantDokument10 SeitenAgreement Between Observed and Interview - Based Exposure To Ergonomics Factors For The Upper Extremities in Employees of A Package Sorting PlantjunholkmNoch keine Bewertungen
- QEC (Quick Exposure Check) : General Description and Development of The MethodDokument4 SeitenQEC (Quick Exposure Check) : General Description and Development of The MethodmulyadiNoch keine Bewertungen
- Ergonomics Study of Automobile-Assembly-LineDokument5 SeitenErgonomics Study of Automobile-Assembly-Linekalite gurusuNoch keine Bewertungen
- Instron Universal Testing MachineDokument12 SeitenInstron Universal Testing MachineGuang Wen Guang WenNoch keine Bewertungen
- Health Risk Evaluation of Whole-Body Vibration by ISO 2631-5 and ISO 2631-1 For Operators of Algricultural Tractor and Recreational VehicleDokument7 SeitenHealth Risk Evaluation of Whole-Body Vibration by ISO 2631-5 and ISO 2631-1 For Operators of Algricultural Tractor and Recreational Vehiclesam_aresNoch keine Bewertungen
- PDF (Published Version)Dokument6 SeitenPDF (Published Version)canavaroyunculukNoch keine Bewertungen
- Musculoskeletal Disorder Risk Assessment in Small Scale Forging Industry by Using RULA MethodDokument6 SeitenMusculoskeletal Disorder Risk Assessment in Small Scale Forging Industry by Using RULA Methodmohitnet1327Noch keine Bewertungen
- Od-2044 Ed.2.2Dokument54 SeitenOd-2044 Ed.2.2Adalnei GomideNoch keine Bewertungen
- Is 10774Dokument14 SeitenIs 10774harshal161987Noch keine Bewertungen
- MAHA USA Complete Product Catalog 2015 071717 PDFDokument31 SeitenMAHA USA Complete Product Catalog 2015 071717 PDFharshal161987Noch keine Bewertungen
- TML LCV & MCV Catalogue Updated On June 2014Dokument136 SeitenTML LCV & MCV Catalogue Updated On June 2014harshal161987Noch keine Bewertungen
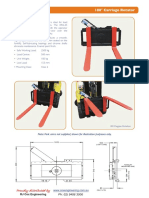
- East West Engineering Forklift AttachmentsDokument39 SeitenEast West Engineering Forklift Attachmentsharshal161987Noch keine Bewertungen
- Fte Kupplungsbroschuere en WebDokument8 SeitenFte Kupplungsbroschuere en Webharshal161987100% (1)
- General Technical PDFDokument40 SeitenGeneral Technical PDFharshal161987Noch keine Bewertungen
- Micro Switch Hdls Limit Ps 002354-1-En FinalDokument39 SeitenMicro Switch Hdls Limit Ps 002354-1-En Finalharshal161987Noch keine Bewertungen
- Is 6051 1970Dokument15 SeitenIs 6051 1970harshal161987100% (1)
- EK Elastomer CouplingsDokument24 SeitenEK Elastomer Couplingsharshal161987Noch keine Bewertungen
- Handbook Longlok PDFDokument48 SeitenHandbook Longlok PDFharshal161987100% (1)
- FD200 FD250Dokument8 SeitenFD200 FD250Tulus Ztx ZaputroNoch keine Bewertungen
- Disclosure To Promote The Right To InformationDokument14 SeitenDisclosure To Promote The Right To Informationharshal161987Noch keine Bewertungen
- 08 Chapter 3Dokument23 Seiten08 Chapter 3Sahaya GrinspanNoch keine Bewertungen
- ch07 PDFDokument17 Seitench07 PDFNarendra Reddy BhumaNoch keine Bewertungen
- Document On Test Method, Testing Equipment and Related ProceduresDokument471 SeitenDocument On Test Method, Testing Equipment and Related Proceduresharshal161987Noch keine Bewertungen
- (14062020 0548) HF Uniform Logo GuidelinesDokument4 Seiten(14062020 0548) HF Uniform Logo GuidelinesBhargaviNoch keine Bewertungen
- Turbine Start-Up SOPDokument17 SeitenTurbine Start-Up SOPCo-gen ManagerNoch keine Bewertungen
- Second Periodical Test in Organization and Management SY 2018-2019Dokument3 SeitenSecond Periodical Test in Organization and Management SY 2018-2019Merida BravoNoch keine Bewertungen
- JCPS School Safety PlanDokument14 SeitenJCPS School Safety PlanDebbie HarbsmeierNoch keine Bewertungen
- Be and Words From The List.: 6B Judging by Appearance Listening and ReadingDokument3 SeitenBe and Words From The List.: 6B Judging by Appearance Listening and ReadingVale MontoyaNoch keine Bewertungen
- Configuring Hyper-V: This Lab Contains The Following Exercises and ActivitiesDokument9 SeitenConfiguring Hyper-V: This Lab Contains The Following Exercises and ActivitiesMD4733566Noch keine Bewertungen
- Emerson Mentor MP ManualDokument182 SeitenEmerson Mentor MP ManualiampedrooNoch keine Bewertungen
- Concrete Casting - Pump Station ADokument13 SeitenConcrete Casting - Pump Station ABright MuzaNoch keine Bewertungen
- Sustainable Development Precautionary PR 2Dokument12 SeitenSustainable Development Precautionary PR 2PramodNoch keine Bewertungen
- Electro TechniquesDokument2 SeitenElectro TechniquesPinkk DaisyfieldNoch keine Bewertungen
- KARAKTERISTIK GEOTERMAL SUMUR EKSPLORASI AT-1, LAPANGAN PANAS BUMI ATADEI, KABUPATEN LEMBATA NTT. Kastiman Sitorus Dan Arif Munandar SUBDIT PANAS BUMIDokument7 SeitenKARAKTERISTIK GEOTERMAL SUMUR EKSPLORASI AT-1, LAPANGAN PANAS BUMI ATADEI, KABUPATEN LEMBATA NTT. Kastiman Sitorus Dan Arif Munandar SUBDIT PANAS BUMIItTo MakinoNoch keine Bewertungen
- Optimizing Stata For Analysis of Large Data SetsDokument29 SeitenOptimizing Stata For Analysis of Large Data SetsTrần Anh TùngNoch keine Bewertungen
- Chapter 3 - Methods of Circuit Analysis and Circuit TheoremsDokument125 SeitenChapter 3 - Methods of Circuit Analysis and Circuit TheoremsNaim NizamNoch keine Bewertungen
- 2018-2019 Annual Algebra Course 1 Contest: InstructionsDokument2 Seiten2018-2019 Annual Algebra Course 1 Contest: InstructionsNaresh100% (1)
- 8051 Programs Using Kit: Exp No: Date: Arithmetic Operations Using 8051Dokument16 Seiten8051 Programs Using Kit: Exp No: Date: Arithmetic Operations Using 8051Gajalakshmi AshokNoch keine Bewertungen
- Bilateral Transfer of LearningDokument18 SeitenBilateral Transfer of Learningts2200419Noch keine Bewertungen
- Handbook On National Spectrum Management 2015Dokument333 SeitenHandbook On National Spectrum Management 2015Marisela AlvarezNoch keine Bewertungen
- Analyst - Finance, John Lewis John Lewis PartnershipDokument2 SeitenAnalyst - Finance, John Lewis John Lewis Partnershipsecret_1992Noch keine Bewertungen
- Operation and Service 69UG15: Diesel Generator SetDokument72 SeitenOperation and Service 69UG15: Diesel Generator Setluis aguileraNoch keine Bewertungen
- 5 Grade: Daily MathDokument130 Seiten5 Grade: Daily MathOLIVEEN WILKS-SCOTT100% (3)
- Pamphlet 89 Chlorine Scrubbing SystemsDokument36 SeitenPamphlet 89 Chlorine Scrubbing Systemshfguavita100% (4)
- Angle ModulationDokument26 SeitenAngle ModulationAtish RanjanNoch keine Bewertungen
- (Word 365-2019) Mos Word MocktestDokument4 Seiten(Word 365-2019) Mos Word MocktestQuỳnh Anh Nguyễn TháiNoch keine Bewertungen
- History of Psychotherapy FinalDokument38 SeitenHistory of Psychotherapy FinalMarco BonettiNoch keine Bewertungen
- GE Uno Downlight Backlit BLDokument2 SeitenGE Uno Downlight Backlit BLChen KengloonNoch keine Bewertungen
- Research Project Presentation of Jobairul Karim ArmanDokument17 SeitenResearch Project Presentation of Jobairul Karim ArmanJobairul Karim ArmanNoch keine Bewertungen
- CNC Milling ReportDokument15 SeitenCNC Milling ReportStarscream Aisyah78% (37)
- Plastic Hinge Length and Depth For Piles in Marine Oil Terminals Including Nonlinear Soil PropertiesDokument10 SeitenPlastic Hinge Length and Depth For Piles in Marine Oil Terminals Including Nonlinear Soil PropertiesGopu RNoch keine Bewertungen
- TinkerPlots Help PDFDokument104 SeitenTinkerPlots Help PDFJames 23fNoch keine Bewertungen
- Car Parking DesignDokument6 SeitenCar Parking Designcharler kinyuajNoch keine Bewertungen
- Functional Safety from Scratch: A Practical Guide to Process Industry ApplicationsVon EverandFunctional Safety from Scratch: A Practical Guide to Process Industry ApplicationsNoch keine Bewertungen
- Guidelines for Initiating Events and Independent Protection Layers in Layer of Protection AnalysisVon EverandGuidelines for Initiating Events and Independent Protection Layers in Layer of Protection AnalysisBewertung: 5 von 5 Sternen5/5 (1)
- The ISO 45001:2018 Implementation Handbook: Guidance on Building an Occupational Health and Safety Management SystemVon EverandThe ISO 45001:2018 Implementation Handbook: Guidance on Building an Occupational Health and Safety Management SystemNoch keine Bewertungen
- Fire Fighting Pumping Systems at Industrial FacilitiesVon EverandFire Fighting Pumping Systems at Industrial FacilitiesBewertung: 4.5 von 5 Sternen4.5/5 (3)
- Healthy Buildings: How Indoor Spaces Drive Performance and ProductivityVon EverandHealthy Buildings: How Indoor Spaces Drive Performance and ProductivityBewertung: 5 von 5 Sternen5/5 (2)
- Redefining Work Health and Safety: Systems, Strategies, and Progressive ApproachesVon EverandRedefining Work Health and Safety: Systems, Strategies, and Progressive ApproachesNoch keine Bewertungen
- A Complete Guide to Safety Officer Interview Questions and AnswersVon EverandA Complete Guide to Safety Officer Interview Questions and AnswersBewertung: 4 von 5 Sternen4/5 (1)
- Plutopia: Nuclear Families, Atomic Cities, and the Great Soviet and American Plutonium DisastersVon EverandPlutopia: Nuclear Families, Atomic Cities, and the Great Soviet and American Plutonium DisastersBewertung: 4 von 5 Sternen4/5 (32)
- Rules of Thumb for Maintenance and Reliability EngineersVon EverandRules of Thumb for Maintenance and Reliability EngineersBewertung: 4.5 von 5 Sternen4.5/5 (12)
- Fundamentals of Risk Management for Process Industry EngineersVon EverandFundamentals of Risk Management for Process Industry EngineersNoch keine Bewertungen
- Epidemiology and Demography in Public HealthVon EverandEpidemiology and Demography in Public HealthJaphet KillewoBewertung: 5 von 5 Sternen5/5 (1)
- Guidelines for Auditing Process Safety Management SystemsVon EverandGuidelines for Auditing Process Safety Management SystemsNoch keine Bewertungen
- Handbook of Hazardous Chemical PropertiesVon EverandHandbook of Hazardous Chemical PropertiesBewertung: 5 von 5 Sternen5/5 (1)
- Introduction to Petroleum Process SafetyVon EverandIntroduction to Petroleum Process SafetyBewertung: 3 von 5 Sternen3/5 (2)
- Electrical Safety Code Manual: A Plain Language Guide to National Electrical Code, OSHA and NFPA 70EVon EverandElectrical Safety Code Manual: A Plain Language Guide to National Electrical Code, OSHA and NFPA 70EBewertung: 3 von 5 Sternen3/5 (6)
- Trevor Kletz Compendium: His Process Safety Wisdom Updated for a New GenerationVon EverandTrevor Kletz Compendium: His Process Safety Wisdom Updated for a New GenerationNoch keine Bewertungen
- What Went Wrong?: Case Histories of Process Plant Disasters and How They Could Have Been AvoidedVon EverandWhat Went Wrong?: Case Histories of Process Plant Disasters and How They Could Have Been AvoidedBewertung: 5 von 5 Sternen5/5 (2)
- Chemical Process Safety: Learning from Case HistoriesVon EverandChemical Process Safety: Learning from Case HistoriesBewertung: 4 von 5 Sternen4/5 (14)
- Culture, Health and Illness: An Introduction for Health ProfessionalsVon EverandCulture, Health and Illness: An Introduction for Health ProfessionalsNoch keine Bewertungen
- Workbook to Accompany Maintenance & Reliability Best PracticesVon EverandWorkbook to Accompany Maintenance & Reliability Best PracticesBewertung: 3.5 von 5 Sternen3.5/5 (3)
- Nutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeVon EverandNutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeNoch keine Bewertungen
- The Invisible Rainbow: A History of Electricity and LifeVon EverandThe Invisible Rainbow: A History of Electricity and LifeBewertung: 4.5 von 5 Sternen4.5/5 (21)