Das könnte Ihnen auch gefallen
- Karay Stock List 11-07-2017 PDFDokument13 SeitenKaray Stock List 11-07-2017 PDFDavid RadovanovicNoch keine Bewertungen
- Karay Stock List 10-10-2017Dokument12 SeitenKaray Stock List 10-10-2017David RadovanovicNoch keine Bewertungen
- Take A Seat Fund RaiserDokument2 SeitenTake A Seat Fund RaiserDavid RadovanovicNoch keine Bewertungen
- 2014 Annual Report - Arm of The SeaDokument2 Seiten2014 Annual Report - Arm of The SeaDavid RadovanovicNoch keine Bewertungen
- Garlic Grower Forms For 2010 Hudson Valley Garlic FestivalDokument9 SeitenGarlic Grower Forms For 2010 Hudson Valley Garlic FestivalDavid RadovanovicNoch keine Bewertungen
- 2013-14 Winter Industrial Supply CatalogDokument12 Seiten2013-14 Winter Industrial Supply CatalogDavid RadovanovicNoch keine Bewertungen
- Hudson Valley Garlic Festival ParkingDokument1 SeiteHudson Valley Garlic Festival ParkingDavid RadovanovicNoch keine Bewertungen
- Karay Metals Stock ListDokument14 SeitenKaray Metals Stock ListDavid RadovanovicNoch keine Bewertungen
- Summer 15 Industrial Supply Promotional CatalogDokument12 SeitenSummer 15 Industrial Supply Promotional CatalogDavid RadovanovicNoch keine Bewertungen
- Industrial Supply Winter 2014 SaleDokument12 SeitenIndustrial Supply Winter 2014 SaleDavid RadovanovicNoch keine Bewertungen
- Food Vendor Forms For 2010 Hudson Valley Garlic FestivalDokument7 SeitenFood Vendor Forms For 2010 Hudson Valley Garlic FestivalDavid RadovanovicNoch keine Bewertungen
- Craft Vendor Forms For 2010 Hudson Valley Garlic FestivalDokument8 SeitenCraft Vendor Forms For 2010 Hudson Valley Garlic FestivalDavid RadovanovicNoch keine Bewertungen
- Ellenville Public Library & Museum Presents INTO THE LIGHTDokument1 SeiteEllenville Public Library & Museum Presents INTO THE LIGHTDavid RadovanovicNoch keine Bewertungen
- Save Saugerties High School Sports - Schedule of EventsDokument1 SeiteSave Saugerties High School Sports - Schedule of EventsDavid RadovanovicNoch keine Bewertungen
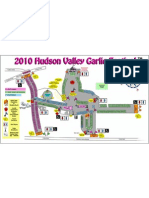
- 2010 Hudson Valley Garlic Festival Map and LayoutDokument1 Seite2010 Hudson Valley Garlic Festival Map and LayoutDavid RadovanovicNoch keine Bewertungen
- Conveyor Belt, Belting and Rubber Hose and Fittings CatalogDokument171 SeitenConveyor Belt, Belting and Rubber Hose and Fittings CatalogDavid Radovanovic100% (1)
- Saugerties Teachers ContractDokument100 SeitenSaugerties Teachers ContractDavid RadovanovicNoch keine Bewertungen
- Business or Packaged Food Vendor Forms For 2010 Hudson Valley Garlic FestivalDokument7 SeitenBusiness or Packaged Food Vendor Forms For 2010 Hudson Valley Garlic FestivalDavid RadovanovicNoch keine Bewertungen
- Industrial Supply and Safety Supplies CatalogDokument308 SeitenIndustrial Supply and Safety Supplies CatalogDavid RadovanovicNoch keine Bewertungen
- March 16, 2010 Saugerties Village BallotDokument1 SeiteMarch 16, 2010 Saugerties Village BallotDavid RadovanovicNoch keine Bewertungen
- Saugerties Occurence Data Unregulated ContaminantsDokument4 SeitenSaugerties Occurence Data Unregulated ContaminantsDavid RadovanovicNoch keine Bewertungen
- Saugerties Teachers' SalariesDokument50 SeitenSaugerties Teachers' SalariesDavid RadovanovicNoch keine Bewertungen
- Saugerties Village Democratic Party Candidates BrochureDokument2 SeitenSaugerties Village Democratic Party Candidates BrochureDavid RadovanovicNoch keine Bewertungen
- Saugerties Voter RegistrationDokument2 SeitenSaugerties Voter RegistrationDavid RadovanovicNoch keine Bewertungen
- Partition Street Project SEQR Negative DeclarationDokument97 SeitenPartition Street Project SEQR Negative DeclarationDavid RadovanovicNoch keine Bewertungen
- Ulster County Planning Board Recommendation For Partition Street Projec T in Saugerties VillageDokument4 SeitenUlster County Planning Board Recommendation For Partition Street Projec T in Saugerties VillageDavid RadovanovicNoch keine Bewertungen
- Spider Barbour Comments On Partition Street Project Pgs. 2,3Dokument2 SeitenSpider Barbour Comments On Partition Street Project Pgs. 2,3David RadovanovicNoch keine Bewertungen
- Spider Barbour Comments On Partition Street Project Pgs. 1Dokument1 SeiteSpider Barbour Comments On Partition Street Project Pgs. 1David RadovanovicNoch keine Bewertungen
- Saugerties Village Democrats Caucus PosterDokument1 SeiteSaugerties Village Democrats Caucus PosterDavid RadovanovicNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- P.S.R. Sadhanantham v. Arunachalam and Anr Article 21: UselessDokument2 SeitenP.S.R. Sadhanantham v. Arunachalam and Anr Article 21: UselessHarsh GuptaNoch keine Bewertungen
- Tindak Pidana Perdagangan Orang Khususnya Terhadap Perempuan Dan Anak: Suatu Permasalahan Dan Penanganannya Di Kota SemarangDokument12 SeitenTindak Pidana Perdagangan Orang Khususnya Terhadap Perempuan Dan Anak: Suatu Permasalahan Dan Penanganannya Di Kota SemarangDiva Pramesti IslamiNoch keine Bewertungen
- Redemption and Termination AgreementDokument4 SeitenRedemption and Termination AgreementJPFNoch keine Bewertungen
- Facts of Vodafone's Case (Case Study)Dokument3 SeitenFacts of Vodafone's Case (Case Study)Nanasaheb MarkadNoch keine Bewertungen
- Executive Branch Test PDFDokument2 SeitenExecutive Branch Test PDFSonyaNoch keine Bewertungen
- 10Dokument15 Seiten10Alhad PingleNoch keine Bewertungen
- 1984 P.CR.L.J 2588Dokument6 Seiten1984 P.CR.L.J 2588Judicial AspirantNoch keine Bewertungen
- Estrada vs. Arroyo Case DigestDokument2 SeitenEstrada vs. Arroyo Case DigestCharmaine Mejia100% (1)
- Agency Reviewer - ArevaloDokument22 SeitenAgency Reviewer - ArevaloAyra ArcillaNoch keine Bewertungen
- Supreme Court upholds election of Yason as Mayor despite turncoatism chargeDokument7 SeitenSupreme Court upholds election of Yason as Mayor despite turncoatism chargeJha NizNoch keine Bewertungen
- 2015 Bar Exam Suggested Answers on Political Law by Bumbo S. CruzDokument18 Seiten2015 Bar Exam Suggested Answers on Political Law by Bumbo S. CruzBumbo S. Cruz100% (1)
- Rule of Law, Human Rights and Judicial Control of Power Some ReflectionsDokument444 SeitenRule of Law, Human Rights and Judicial Control of Power Some ReflectionsasdfNoch keine Bewertungen
- URBANES vs SECRETARY Case DigestDokument3 SeitenURBANES vs SECRETARY Case Digestchappy_leigh118Noch keine Bewertungen
- Court upholds Torrens title despite lack of personal noticeDokument1 SeiteCourt upholds Torrens title despite lack of personal noticeShammah Rey Mahinay100% (1)
- En Banc (G.R. No. 116437. March 3, 1997.)Dokument15 SeitenEn Banc (G.R. No. 116437. March 3, 1997.)Jason CruzNoch keine Bewertungen
- Jonathan Maldonado-Perez Probable Cause StatementDokument2 SeitenJonathan Maldonado-Perez Probable Cause StatementAdam ForgieNoch keine Bewertungen
- Provident Insurance vs. Ca FactsDokument39 SeitenProvident Insurance vs. Ca FactsCrestu JinNoch keine Bewertungen
- Heirs of Eugenio Lopez, Sr. vs. EnriquezDokument1 SeiteHeirs of Eugenio Lopez, Sr. vs. EnriquezEllah GaudicosNoch keine Bewertungen
- Ethical Values (Animal Experimentation) Reading ComprehensionDokument5 SeitenEthical Values (Animal Experimentation) Reading ComprehensionsigugiNoch keine Bewertungen
- I Am Sharing 'Bar Ops 2' With YouDokument27 SeitenI Am Sharing 'Bar Ops 2' With YouYsabelleNoch keine Bewertungen
- Cases Transpo MidtermsDokument42 SeitenCases Transpo MidtermsAnnKhoLugasanNoch keine Bewertungen
- Software Maintenance AgreementDokument4 SeitenSoftware Maintenance AgreementAmardeep Singh HudaNoch keine Bewertungen
- GR# 189655Dokument10 SeitenGR# 189655Simeon SuanNoch keine Bewertungen
- Yellow JournalismDokument14 SeitenYellow Journalismtaasha26Noch keine Bewertungen
- Annexure GLDokument3 SeitenAnnexure GLNitinAgnihotri41% (17)
- Intentional Torts and Defences ExplainedDokument3 SeitenIntentional Torts and Defences ExplainedMarc MNoch keine Bewertungen
- GO - Ms.No.13 Dt.15.Dokument5 SeitenGO - Ms.No.13 Dt.15.Rajesh Babu50% (2)
- Strategic Alliance vs. Radstock Securities PDFDokument2 SeitenStrategic Alliance vs. Radstock Securities PDFrapgracelim100% (1)
- MIAA v. AirspanDokument11 SeitenMIAA v. AirspanIldefonso HernaezNoch keine Bewertungen
- Grand Boulevard Hotel v. Genuine Labor OrganizationDokument2 SeitenGrand Boulevard Hotel v. Genuine Labor OrganizationAnonymous 5MiN6I78I0100% (1)