Das könnte Ihnen auch gefallen
- RH Blood Group System MazenDokument36 SeitenRH Blood Group System MazenOsama Bakheet100% (3)
- Psychology of Eating DisorderDokument13 SeitenPsychology of Eating DisorderPsych2GoNoch keine Bewertungen
- Session 8Dokument6 SeitenSession 8madcalNoch keine Bewertungen
- Immunohematology+I+Lecture+6+Rh+continued 1Dokument20 SeitenImmunohematology+I+Lecture+6+Rh+continued 1tamiqua1Noch keine Bewertungen
- RH Blood Group SystemDokument61 SeitenRH Blood Group SystemValdez Francis ZaccheauNoch keine Bewertungen
- Dr. TT - 2019 AntiRhesusDokument36 SeitenDr. TT - 2019 AntiRhesusIrsan SirajuddinNoch keine Bewertungen
- RH Blood Group System: Group 10: Tambasacan, Tomaro, Villanueva, Valdez, YabesDokument62 SeitenRH Blood Group System: Group 10: Tambasacan, Tomaro, Villanueva, Valdez, YabesValdez Francis ZaccheauNoch keine Bewertungen
- Blood GroupingDokument27 SeitenBlood Groupingfatimanasir2266Noch keine Bewertungen
- Blood Groups: Dr. Kenan GumustekinDokument43 SeitenBlood Groups: Dr. Kenan Gumustekinsyed nomanshahNoch keine Bewertungen
- Physio. D. Suroor L3 Blood Typing& TransfusionDokument19 SeitenPhysio. D. Suroor L3 Blood Typing& TransfusionAhmed OudahNoch keine Bewertungen
- Blood Group NewDokument44 SeitenBlood Group NewArpita SankhwarNoch keine Bewertungen
- 2 - RH SystemDokument12 Seiten2 - RH Systemجير يكو (جيريكو)Noch keine Bewertungen
- Blood Grouping 1690574753Dokument30 SeitenBlood Grouping 1690574753willowmaecayabyabNoch keine Bewertungen
- Blood Group & RHDokument27 SeitenBlood Group & RHfamtaluNoch keine Bewertungen
- 13 Other Blood Group SystemsDokument56 Seiten13 Other Blood Group SystemsCarinaJongLeeNoch keine Bewertungen
- RH TypingDokument5 SeitenRH TypingHannah Alonzo VirtudazoNoch keine Bewertungen
- ABO and RH Blood Group SystemDokument31 SeitenABO and RH Blood Group SystemKaab Ishaq100% (1)
- RH GroupDokument11 SeitenRH GroupJhon WickNoch keine Bewertungen
- Lecture On Blood Groups, Transfusion, RH Incompatibility by Dr. RoomiDokument41 SeitenLecture On Blood Groups, Transfusion, RH Incompatibility by Dr. RoomiMudassar Roomi100% (1)
- Blood GroupingDokument84 SeitenBlood GroupingUday KolheNoch keine Bewertungen
- Hemolytic Disease of The NewbornDokument16 SeitenHemolytic Disease of The NewbornStanculescu MarianaNoch keine Bewertungen
- Blood Bank and Blood TransfusionDokument11 SeitenBlood Bank and Blood TransfusionMostafa Adel Ahmd100% (1)
- Dr. Husnil Kadri, M.KesDokument44 SeitenDr. Husnil Kadri, M.KesElsa Giatri SiradjNoch keine Bewertungen
- Week 9-Other Blood Group System-Part 2 PDFDokument37 SeitenWeek 9-Other Blood Group System-Part 2 PDFjohn carlo cabanlitNoch keine Bewertungen
- 4BBK Lec4 - RH Group MQA 2019-09-26 08 - 14 - 36Dokument33 Seiten4BBK Lec4 - RH Group MQA 2019-09-26 08 - 14 - 36gothai sivapragasamNoch keine Bewertungen
- Transfusion MedicineDokument13 SeitenTransfusion MedicineTina MultazamiNoch keine Bewertungen
- Rhesus SystemDokument41 SeitenRhesus SystemLaud ArthurNoch keine Bewertungen
- 5.Rh Blood Group SystemDokument22 Seiten5.Rh Blood Group Systemjong188Noch keine Bewertungen
- Lecture10 - Blood Groups and TransfusionDokument28 SeitenLecture10 - Blood Groups and Transfusionmohapatrarashmi050Noch keine Bewertungen
- RH IncompatibilityDokument38 SeitenRH IncompatibilitySagun lohalaNoch keine Bewertungen
- Is BB Final Coaching NotesDokument8 SeitenIs BB Final Coaching NotesLeomill MendiolaNoch keine Bewertungen
- Blood Bank IIIDokument72 SeitenBlood Bank IIIPerlie CNoch keine Bewertungen
- Hemolytic Disease of Newborn Class NotesDokument37 SeitenHemolytic Disease of Newborn Class NotesElvisNoch keine Bewertungen
- Rhesus Blood Group System: NotesDokument10 SeitenRhesus Blood Group System: NotesAarzoo SikarwarNoch keine Bewertungen
- Management of Pregnancy Complicated by Rhesus (D) Alloimmunization IIDokument6 SeitenManagement of Pregnancy Complicated by Rhesus (D) Alloimmunization IIlobomhNoch keine Bewertungen
- Positive Direct Antiglobulin Test and Autoimmune Hemolytic AnemiasDokument30 SeitenPositive Direct Antiglobulin Test and Autoimmune Hemolytic AnemiasFirsty Demy ChristantiNoch keine Bewertungen
- Du TestDokument14 SeitenDu TestlalhaiagustinNoch keine Bewertungen
- Pocket Guide On Red Cells 2012Dokument8 SeitenPocket Guide On Red Cells 2012Dave OrlandoNoch keine Bewertungen
- Lec6 Sem7 RepWK6 20140417Dokument6 SeitenLec6 Sem7 RepWK6 20140417watchthestarkNoch keine Bewertungen
- Blood Groups: DR - Agus Alim Abdullah, SPPK (K)Dokument60 SeitenBlood Groups: DR - Agus Alim Abdullah, SPPK (K)wahyuniNoch keine Bewertungen
- Blood Transfusion: Moderator: DR - Ibrahim Qudaisat Presented by Murad SataryDokument46 SeitenBlood Transfusion: Moderator: DR - Ibrahim Qudaisat Presented by Murad SataryMorad SatariNoch keine Bewertungen
- Human Blood GroupsDokument29 SeitenHuman Blood GroupsKunalNoch keine Bewertungen
- MD2011 HRM Week 3 Transfusion Medicine ViewDokument40 SeitenMD2011 HRM Week 3 Transfusion Medicine ViewShiv SookunNoch keine Bewertungen
- RH Blood Group SystemDokument18 SeitenRH Blood Group SystemChristian John Mabalot Carillo50% (2)
- DR - Jaisankar.P.: Blood Grouping and Transfusion TherapyDokument63 SeitenDR - Jaisankar.P.: Blood Grouping and Transfusion TherapyDrSanjeev ShrivastavaNoch keine Bewertungen
- Blood Types & TransfusionDokument20 SeitenBlood Types & TransfusionDr Imran AftabNoch keine Bewertungen
- RH IsoimmunizationDokument15 SeitenRH Isoimmunizationgeorgeloto12Noch keine Bewertungen
- الطب الباطني ع2 ك2Dokument4 Seitenالطب الباطني ع2 ك2Hassan EssaNoch keine Bewertungen
- RH Debil DuDokument4 SeitenRH Debil DuMaria Chacón CarbajalNoch keine Bewertungen
- Blood TransfusionDokument19 SeitenBlood Transfusion10-AKASH MNoch keine Bewertungen
- Haemolytic Disease of The NewbornDokument46 SeitenHaemolytic Disease of The Newborntan_kit_1100% (1)
- Blood GroupingDokument35 SeitenBlood GroupingSUNIL KUMARNoch keine Bewertungen
- Antigen RhesusDokument30 SeitenAntigen Rhesusarmada thamNoch keine Bewertungen
- Lab 5Dokument22 SeitenLab 5Aveen MustafaNoch keine Bewertungen
- Blood Transfusion: Study GuideDokument22 SeitenBlood Transfusion: Study GuideAnnabelle KingfulNoch keine Bewertungen
- TP Immunology English 2018 For StudentDokument83 SeitenTP Immunology English 2018 For StudentKhaled Abo Al OyounNoch keine Bewertungen
- Blood Groups: 1 PhysiologyDokument36 SeitenBlood Groups: 1 PhysiologyAkash JaatNoch keine Bewertungen
- Chpt. 7 BlanksDokument19 SeitenChpt. 7 BlanksmoonrakerwiskNoch keine Bewertungen
- RH System PPDokument38 SeitenRH System PPتجربة أولىNoch keine Bewertungen
- 3rh 2Dokument38 Seiten3rh 2Fuentes, Jade Andrey R. BSMT 2-ANoch keine Bewertungen
- Pattern - 3D Crochet HeartDokument3 SeitenPattern - 3D Crochet Heartjong188100% (1)
- Diagrammatic Summary of Two Sample TestsDokument1 SeiteDiagrammatic Summary of Two Sample TestsCarina JLNoch keine Bewertungen
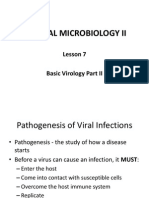
- Medical Microbiology II Lecture 8Dokument53 SeitenMedical Microbiology II Lecture 8jong188100% (1)
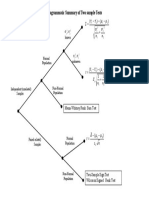
- Diagrammatic Summary of Three Sample TestsDokument1 SeiteDiagrammatic Summary of Three Sample TestsCarina JLNoch keine Bewertungen
- Medical Microbiology II Lecture 12Dokument62 SeitenMedical Microbiology II Lecture 12jong188Noch keine Bewertungen
- Medical Microbiology II Lecture 7Dokument77 SeitenMedical Microbiology II Lecture 7jong188Noch keine Bewertungen
- Medical Microbiology II Lecture 11Dokument31 SeitenMedical Microbiology II Lecture 11jong188Noch keine Bewertungen
- Medical Microbiology II Lecture 10Dokument64 SeitenMedical Microbiology II Lecture 10jong188Noch keine Bewertungen
- Dengue Fever Asignment 25.11.11Dokument5 SeitenDengue Fever Asignment 25.11.11jong188Noch keine Bewertungen
- 5.Rh Blood Group SystemDokument22 Seiten5.Rh Blood Group Systemjong188Noch keine Bewertungen
- Medical Microbiology II Lecture 9Dokument65 SeitenMedical Microbiology II Lecture 9jong188Noch keine Bewertungen
- 4.isoantibodies of ABO SystemDokument32 Seiten4.isoantibodies of ABO SystemCarinaTingEeNoch keine Bewertungen
- ABO Typing ProcedureDokument29 SeitenABO Typing Procedurejong188Noch keine Bewertungen
- ABO Blood GroupDokument42 SeitenABO Blood Groupjong188Noch keine Bewertungen
- Intro To ImmunohematoDokument48 SeitenIntro To Immunohematojong188Noch keine Bewertungen
- Zoonotic Diseases - Laboratory RabbitsDokument2 SeitenZoonotic Diseases - Laboratory RabbitsramperoughNoch keine Bewertungen
- IcdDokument1.590 SeitenIcdZainalAbidinNoch keine Bewertungen
- Checklist For Enrollment of ProvidersDokument7 SeitenChecklist For Enrollment of ProvidersMaria Crayton HaliburtonNoch keine Bewertungen
- Gavage Feeding RepDokument6 SeitenGavage Feeding RepEon Provido AlfaroNoch keine Bewertungen
- Recalls 3Dokument26 SeitenRecalls 3Charisse CaydanNoch keine Bewertungen
- Chapter 9: Congenital Constriction Band Syndrome (CCBS)Dokument3 SeitenChapter 9: Congenital Constriction Band Syndrome (CCBS)Javaid KhanNoch keine Bewertungen
- Prevalence of Depression, Anxiety, and Associated Factors in Residents From Hospital Centers During COVID-19 PandemicDokument6 SeitenPrevalence of Depression, Anxiety, and Associated Factors in Residents From Hospital Centers During COVID-19 PandemicMericia Guadalupe Sandoval ChavezNoch keine Bewertungen
- CLIAProf Testing Booklet FINALrevDokument12 SeitenCLIAProf Testing Booklet FINALrevgaber 230Noch keine Bewertungen
- Flu Specimen Collection PosterDokument1 SeiteFlu Specimen Collection Poster568563Noch keine Bewertungen
- Chist de Septum PellucidumDokument3 SeitenChist de Septum PellucidumdansarariuNoch keine Bewertungen
- Berra 2020Dokument12 SeitenBerra 2020Indri AswariNoch keine Bewertungen
- AdamRouilly Healthcare Education Catalogue 2015-16Dokument326 SeitenAdamRouilly Healthcare Education Catalogue 2015-16NGUYEN HUU TRUONG TruongNoch keine Bewertungen
- MANIFESTASI KLINIK Penyakit Jantung KoronerDokument4 SeitenMANIFESTASI KLINIK Penyakit Jantung KoronerDwitya NoviariNoch keine Bewertungen
- Bacterial MeningitisDokument2 SeitenBacterial MeningitisSpideyPacerNoch keine Bewertungen
- Lyrica - Prescribing InfoDokument42 SeitenLyrica - Prescribing InfoPoojaNoch keine Bewertungen
- Medical Equipment Technology I: Joseph Asamoah-AsareDokument22 SeitenMedical Equipment Technology I: Joseph Asamoah-AsareNyuori CosmasNoch keine Bewertungen
- The Format: Case Study FormDokument17 SeitenThe Format: Case Study FormJane DyNoch keine Bewertungen
- Manual Monitor Criticare Sholar IIIDokument90 SeitenManual Monitor Criticare Sholar IIIandres narvaezNoch keine Bewertungen
- BodyBallancer Lipo Brochure PDFDokument2 SeitenBodyBallancer Lipo Brochure PDFRoss Gale100% (1)
- Palicka Simpozion Management RiscDokument60 SeitenPalicka Simpozion Management Risccornelialautarescu6411Noch keine Bewertungen
- Please Stand by ..: © Business & Legal Reports, Inc. 1110Dokument37 SeitenPlease Stand by ..: © Business & Legal Reports, Inc. 1110Johanamhy PanergoNoch keine Bewertungen
- Red Tide: Causative AgentDokument2 SeitenRed Tide: Causative Agentchristian quiaoitNoch keine Bewertungen
- Labreportnew 6782Dokument1 SeiteLabreportnew 6782Shahabuddin AnsariNoch keine Bewertungen
- Autonomic Dysreflexia-Part OneDokument3 SeitenAutonomic Dysreflexia-Part OneManuel BucurNoch keine Bewertungen
- Amenorrhoea RemediesDokument8 SeitenAmenorrhoea RemediesHomeopathy TorrentsNoch keine Bewertungen
- Basic Need For GeriatricsDokument38 SeitenBasic Need For GeriatricsMuhammad Yatsrib SemmeNoch keine Bewertungen
- Glossopharyngeal Nerve Injury Following Tonsillectomy 5542Dokument4 SeitenGlossopharyngeal Nerve Injury Following Tonsillectomy 5542Kenza SeddikNoch keine Bewertungen
- Ann Blake SSRI DepressionDokument17 SeitenAnn Blake SSRI Depressionthings3100% (1)
- Clinical Medical Reviews and Case Reports CMRCR 5 227Dokument8 SeitenClinical Medical Reviews and Case Reports CMRCR 5 227Juan BacelarNoch keine Bewertungen