Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Presentation (Final)Dokument32 SeitenPresentation (Final)Sarah Rose FeccoNoch keine Bewertungen
- Case ReportDokument11 SeitenCase ReportBerhanu DigamoNoch keine Bewertungen
- Physical Abuse Teaching SlidesDokument19 SeitenPhysical Abuse Teaching SlidesbentoeNoch keine Bewertungen
- Arterial Blood Gas AnalysisDokument24 SeitenArterial Blood Gas AnalysisDeepika PatelNoch keine Bewertungen
- Textbook of Gynaecological OncologyDokument58 SeitenTextbook of Gynaecological OncologyMarco Vinicio Benavides Osorto100% (2)
- Seminar: Pere Ginès, Aleksander Krag, Juan G Abraldes, Elsa Solà, Núria Fabrellas, Patrick S KamathDokument18 SeitenSeminar: Pere Ginès, Aleksander Krag, Juan G Abraldes, Elsa Solà, Núria Fabrellas, Patrick S KamathcastillojessNoch keine Bewertungen
- Radiologi Gastrointestinal (Noted)Dokument52 SeitenRadiologi Gastrointestinal (Noted)desak 102018084Noch keine Bewertungen
- Complications of Insulin TherapyDokument16 SeitenComplications of Insulin TherapyIngrid NicolasNoch keine Bewertungen
- Icru 89 (229-260)Dokument32 SeitenIcru 89 (229-260)Christian Ordoñez100% (1)
- Treatment Modalities Applicable To The Psychiatric ClientDokument53 SeitenTreatment Modalities Applicable To The Psychiatric Clientnickybore100% (1)
- Bioengineering Transla Med - 2022 - Chopade - Alzheimer S and Parkinson S Disease Therapies in The ClinicDokument23 SeitenBioengineering Transla Med - 2022 - Chopade - Alzheimer S and Parkinson S Disease Therapies in The ClinicurosNoch keine Bewertungen
- Drugs Used in Heart FailureDokument33 SeitenDrugs Used in Heart FailureLynx Kee Bayating100% (1)
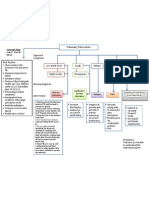
- Concept Map PTBDokument1 SeiteConcept Map PTBJoan Abardo100% (2)
- Exercise #1 10Dokument10 SeitenExercise #1 10John Paul FloresNoch keine Bewertungen
- Mental IllnessDokument3 SeitenMental IllnessKate EvangelistaNoch keine Bewertungen
- Gujarat Technological University: W.E.F. AY 2017-18Dokument3 SeitenGujarat Technological University: W.E.F. AY 2017-18raj royelNoch keine Bewertungen
- Diabetic Nephropathy BaruDokument24 SeitenDiabetic Nephropathy BaruRobiyanti Nur Chalifah HattaNoch keine Bewertungen
- Manual of Bone Densitometry Measurements - An Aid To The Interpretation of Bone Densitometry Measurements in A Clinical Setting PDFDokument229 SeitenManual of Bone Densitometry Measurements - An Aid To The Interpretation of Bone Densitometry Measurements in A Clinical Setting PDFsesjrsNoch keine Bewertungen
- PediatricsDokument312 SeitenPediatricsمحمد ابو مناضل الافينش100% (1)
- Extravasation Neutral (Non-Irritant) Irritant Irritant With Vesicant Properties VesicantsDokument12 SeitenExtravasation Neutral (Non-Irritant) Irritant Irritant With Vesicant Properties VesicantsmarcNoch keine Bewertungen
- Repair of HydroceleDokument20 SeitenRepair of HydroceleNatanael AdiNoch keine Bewertungen
- Celiac DiseaseDokument5 SeitenCeliac DiseaseJhevey ValdezNoch keine Bewertungen
- @MBS MedicalBooksStore 2020 CompressionDokument46 Seiten@MBS MedicalBooksStore 2020 CompressionTaufikNoch keine Bewertungen
- Elevated Levels of Bcl-3 Inhibits Treg Development and Function Resulting in Spontaneous ColitisDokument14 SeitenElevated Levels of Bcl-3 Inhibits Treg Development and Function Resulting in Spontaneous ColitisPaviliuc RalucaNoch keine Bewertungen
- New Health Care Clinical: Laboratory SrinagarDokument1 SeiteNew Health Care Clinical: Laboratory SrinagarRajaNoch keine Bewertungen
- Kleptomania Term PaperDokument6 SeitenKleptomania Term Paperbctfnerif100% (1)
- Suicide in Adolescent - A Case ReportDokument5 SeitenSuicide in Adolescent - A Case ReportRebecca SilaenNoch keine Bewertungen
- Measuring Central Venous Pressure: Elaine ColeDokument8 SeitenMeasuring Central Venous Pressure: Elaine ColednllkzaNoch keine Bewertungen
- Congestion Pelvica 2020Dokument6 SeitenCongestion Pelvica 2020Cristian RodríguezNoch keine Bewertungen
- Patient Information Leaflet: (Etonogestrel)Dokument4 SeitenPatient Information Leaflet: (Etonogestrel)A VHRSENoch keine Bewertungen