Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Orthopaedic Electives: Clerkship Coordinator: Amanda SchwanzDokument34 SeitenOrthopaedic Electives: Clerkship Coordinator: Amanda SchwanzvimalNoch keine Bewertungen
- INTANDokument2 SeitenINTANvimalNoch keine Bewertungen
- Director &HOD Prof - Dr. K.PRAKASAM M.S.Ortho, D.Ortho, DSC (Hon)Dokument70 SeitenDirector &HOD Prof - Dr. K.PRAKASAM M.S.Ortho, D.Ortho, DSC (Hon)vimalNoch keine Bewertungen
- Surgical Wound, Surgical Site Infection and AbxDokument53 SeitenSurgical Wound, Surgical Site Infection and AbxvimalNoch keine Bewertungen
- 328 - Management of Polytrauma PatientDokument62 Seiten328 - Management of Polytrauma PatientvimalNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Narcism Ronningstam1996Dokument15 SeitenNarcism Ronningstam1996Angela EnacheNoch keine Bewertungen
- Geriatric Depression ScaleDokument10 SeitenGeriatric Depression Scalesneha dasNoch keine Bewertungen
- Unsupervised Learning Networks: "Principles of Soft Computing, 2Dokument44 SeitenUnsupervised Learning Networks: "Principles of Soft Computing, 2جرح الماضيNoch keine Bewertungen
- Research and Symposia Abstracts From The Congress of The InternationalDokument20 SeitenResearch and Symposia Abstracts From The Congress of The InternationaldrguillermomedinaNoch keine Bewertungen
- Perceiving Acoustic Source Orientation in Three-Dimensional SpaceDokument6 SeitenPerceiving Acoustic Source Orientation in Three-Dimensional SpaceMaria SuterNoch keine Bewertungen
- Conscious Memory Recall (Soul Fragment Retrievel)Dokument12 SeitenConscious Memory Recall (Soul Fragment Retrievel)GlennPendleton80% (5)
- Cybor: Donald A. NormanDokument3 SeitenCybor: Donald A. Normanfreiheit137174Noch keine Bewertungen
- Eggermont 2019 ABRDokument15 SeitenEggermont 2019 ABRSujeet PathakNoch keine Bewertungen
- Developmental Coordination DisorderDokument4 SeitenDevelopmental Coordination DisorderAmmar-1996Noch keine Bewertungen
- Cerebral PalsyDokument40 SeitenCerebral PalsyStefan ChrisnawanNoch keine Bewertungen
- Literatür 1Dokument6 SeitenLiteratür 1Oguzhan KumNoch keine Bewertungen
- Where To Place Your TENS PadsDokument8 SeitenWhere To Place Your TENS PadsKailyne WatersNoch keine Bewertungen
- A. Content Standards: I. ObjectivesDokument7 SeitenA. Content Standards: I. ObjectivesRahil MamberingNoch keine Bewertungen
- Physical Rehabilitation 6th Edition Osullivan Test BankDokument4 SeitenPhysical Rehabilitation 6th Edition Osullivan Test Bankkristinaspencerwnpqmgifrs100% (34)
- Metacognitie Si MindfulnessDokument17 SeitenMetacognitie Si MindfulnessdanacurtNoch keine Bewertungen
- Pop Quiz Nervous SystemDokument5 SeitenPop Quiz Nervous Systemapi-242868690100% (1)
- Chapter 104:: Psychocutaneous Skin Disease:: Evan Rieder & Francisco A. TauskDokument9 SeitenChapter 104:: Psychocutaneous Skin Disease:: Evan Rieder & Francisco A. TauskLaras KinasihNoch keine Bewertungen
- JSSU B.pharm Regulation and Syllabus 2012Dokument95 SeitenJSSU B.pharm Regulation and Syllabus 2012vkguptajssNoch keine Bewertungen
- 1715 StewartDokument43 Seiten1715 StewartRafael AlvesNoch keine Bewertungen
- Leaky Gut in AutismDokument18 SeitenLeaky Gut in AutismAdinda RaihanaNoch keine Bewertungen
- Time - The Science of Memory - 2019 PDFDokument99 SeitenTime - The Science of Memory - 2019 PDFCarlos Carreño100% (2)
- Dandy WalkerDokument12 SeitenDandy WalkerzarithNoch keine Bewertungen
- Initial Evaluation Consultation Chief Complaint: Name: History of Present Illness: RoomDokument4 SeitenInitial Evaluation Consultation Chief Complaint: Name: History of Present Illness: RoomwhitneyagNoch keine Bewertungen
- Introduction To Autonomic PharmacologyDokument55 SeitenIntroduction To Autonomic PharmacologyMuammar Alfarouq100% (1)
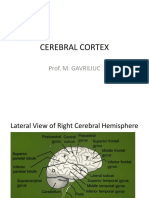
- 13 Cerebral CortexDokument85 Seiten13 Cerebral CortexIon UngureanuNoch keine Bewertungen
- Chapter Orofacial PainDokument34 SeitenChapter Orofacial PainintanNoch keine Bewertungen
- Patient and Family Guide To The CANMAT and ISBD Guidelines On The Management of Bipolar DisorderDokument34 SeitenPatient and Family Guide To The CANMAT and ISBD Guidelines On The Management of Bipolar DisorderLucila VialeNoch keine Bewertungen
- Physio Neuro Ax TemplateDokument8 SeitenPhysio Neuro Ax TemplateHussain LaftaNoch keine Bewertungen
- Sub - Medical Surgical Nursing: Assignment On Neurological AssessmentDokument11 SeitenSub - Medical Surgical Nursing: Assignment On Neurological Assessmentkamini Choudhary100% (1)
- Hypnosis For Chronic Pain Management - Wo - Mark P. JensenDokument160 SeitenHypnosis For Chronic Pain Management - Wo - Mark P. Jensenseveruspiton980% (5)