Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Algo Postarrest PDFDokument1 SeiteAlgo Postarrest PDFdewita wahyu kemalasariNoch keine Bewertungen
- Minor Diagnostic CriteriaDokument3 SeitenMinor Diagnostic CriteriaMediatrix OhoiwirinNoch keine Bewertungen
- Algo AcsDokument1 SeiteAlgo AcsMediatrix OhoiwirinNoch keine Bewertungen
- Algo Acs PDFDokument1 SeiteAlgo Acs PDFNety Pandung SalembanNoch keine Bewertungen
- Eng PDFDokument302 SeitenEng PDFAnonymous YdFUaW6fBNoch keine Bewertungen
- Minor Diagnostic CriteriaDokument3 SeitenMinor Diagnostic CriteriaMediatrix OhoiwirinNoch keine Bewertungen
- Daftar PustakaDokument3 SeitenDaftar PustakaMediatrix OhoiwirinNoch keine Bewertungen
- Epidural Steroid InjectionsDokument48 SeitenEpidural Steroid InjectionsMediatrix OhoiwirinNoch keine Bewertungen
- Nutrients-04-01042Dokument16 SeitenNutrients-04-01042Mediatrix OhoiwirinNoch keine Bewertungen
- 278 Management of Paediatric Sepsis PDFDokument10 Seiten278 Management of Paediatric Sepsis PDFAfrizal AdzNoch keine Bewertungen
- Mobile Phone Use and Risk of Tumors: A Meta-Analysis: Ournal of Linical NcologyDokument8 SeitenMobile Phone Use and Risk of Tumors: A Meta-Analysis: Ournal of Linical NcologyMediatrix OhoiwirinNoch keine Bewertungen
- J Neurol Neurosurg Psychiatry 2004 Manji I29 35Dokument9 SeitenJ Neurol Neurosurg Psychiatry 2004 Manji I29 35Mediatrix OhoiwirinNoch keine Bewertungen
- Csa Prot 2013Dokument60 SeitenCsa Prot 2013Mediatrix OhoiwirinNoch keine Bewertungen
- Taj Pharma's FDA-Approved Generic Version, Cisplatin InjectionDokument1 SeiteTaj Pharma's FDA-Approved Generic Version, Cisplatin InjectionTAJ PHARMA — A Health Care ProviderNoch keine Bewertungen
- 1 Anti Emetics II BDS 3 June 2020 AdobeDokument28 Seiten1 Anti Emetics II BDS 3 June 2020 AdobeBishal ChauhanNoch keine Bewertungen
- Popis Bolesti, Kod Kojih Liječenje Zapperom Daje Pozitivni RezultatDokument7 SeitenPopis Bolesti, Kod Kojih Liječenje Zapperom Daje Pozitivni RezultatMićo RadenovićNoch keine Bewertungen
- Abdominal SonographyDokument6 SeitenAbdominal SonographyRio FutabaNoch keine Bewertungen
- Pharmanutrition: Yoichi Sunagawa, Yasufumi Katanasaka, Koji Hasegawa, Tatsuya MorimotoDokument5 SeitenPharmanutrition: Yoichi Sunagawa, Yasufumi Katanasaka, Koji Hasegawa, Tatsuya MorimotoRizky AmaliaNoch keine Bewertungen
- DIPHTHERIADokument12 SeitenDIPHTHERIANununNoch keine Bewertungen
- Ketoconazole Cream Clinical ParticularsDokument2 SeitenKetoconazole Cream Clinical ParticularsJai MurugeshNoch keine Bewertungen
- Causes of Ischemic Stroke: October 2010Dokument19 SeitenCauses of Ischemic Stroke: October 2010Pajokka 10Noch keine Bewertungen
- Psychiatry HistoryDokument53 SeitenPsychiatry HistoryMarco Góis100% (5)
- DRUG STUDY (Mefenamic Acid)Dokument4 SeitenDRUG STUDY (Mefenamic Acid)Paolo Digo67% (6)
- DR MITIC Herbal Drops Store Product Catalog ENGLISH 31.03.2019Dokument30 SeitenDR MITIC Herbal Drops Store Product Catalog ENGLISH 31.03.2019Dacan MiticNoch keine Bewertungen
- Hema 1 ErythropoiesisDokument20 SeitenHema 1 Erythropoiesismarie judimor gomezNoch keine Bewertungen
- High Anion Gap Metabolic AcidosisDokument6 SeitenHigh Anion Gap Metabolic AcidosisharvardboyNoch keine Bewertungen
- Penis & DisordersDokument54 SeitenPenis & Disordersshivay100% (1)
- Materi Praktikum Pap Smear Modul ReproduksiDokument77 SeitenMateri Praktikum Pap Smear Modul Reproduksisusilorini100% (10)
- Syringomyelia, Arachnoiditis and SpasticityDokument53 SeitenSyringomyelia, Arachnoiditis and SpasticitySam OlukaNoch keine Bewertungen
- August 03 2017 Recalls Mls (Ascpi)Dokument6 SeitenAugust 03 2017 Recalls Mls (Ascpi)Joanna Carel Lopez100% (3)
- Jurnal Condyloma AcuminataDokument11 SeitenJurnal Condyloma Acuminataperussi pranadiptaNoch keine Bewertungen
- Neuro UrologyDokument53 SeitenNeuro UrologymoominjunaidNoch keine Bewertungen
- Ebook Cultural Anthropology Canadian 2Nd Edition Robbins Test Bank Full Chapter PDFDokument34 SeitenEbook Cultural Anthropology Canadian 2Nd Edition Robbins Test Bank Full Chapter PDFengagerscotsmangk9jt100% (8)
- The Term Aplastic Anemia Indicates: Pancytopenia in The PresenceDokument34 SeitenThe Term Aplastic Anemia Indicates: Pancytopenia in The PresenceKhadar mohamedNoch keine Bewertungen
- Environmental SanitationDokument25 SeitenEnvironmental SanitationAlessandra Marigold Aguilar PerezNoch keine Bewertungen
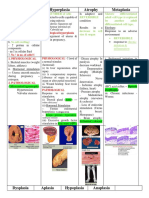
- Hypertrophy Hyperplasia Atrophy MetaplasiaDokument20 SeitenHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNoch keine Bewertungen
- ClubfootDokument4 SeitenClubfootDaphne AleliNoch keine Bewertungen
- Case Study GonorrheaDokument19 SeitenCase Study GonorrheaErika ThereseNoch keine Bewertungen
- 2 Newborn AssesmentDokument23 Seiten2 Newborn Assesment.Noch keine Bewertungen
- Interest of Early Toxicological Sampling During Alpha Chloralose in Toxication, A Case ReportDokument4 SeitenInterest of Early Toxicological Sampling During Alpha Chloralose in Toxication, A Case ReportIJAR JOURNALNoch keine Bewertungen
- Hypertensive Disorder in PregnancyDokument7 SeitenHypertensive Disorder in PregnancyBiscuits and milkNoch keine Bewertungen
- Script AbdomenDokument19 SeitenScript AbdomenRespicio Christian Aejay G.Noch keine Bewertungen
- Review Notes 2000 - Geriatrics PDFDokument12 SeitenReview Notes 2000 - Geriatrics PDFeset5Noch keine Bewertungen