Das könnte Ihnen auch gefallen
- FRAMECAD F300i Operating Manual (FCF2) - Release 10102013Dokument221 SeitenFRAMECAD F300i Operating Manual (FCF2) - Release 10102013assssaaassd100% (4)
- Design and Evaluation of Inflatable Wings For UavsDokument290 SeitenDesign and Evaluation of Inflatable Wings For UavsmegustalazorraNoch keine Bewertungen
- Polymer TestingDokument201 SeitenPolymer TestingAl-Kawthari As-Sunni100% (8)
- Statistical Process Control & Cost of QualityDokument114 SeitenStatistical Process Control & Cost of QualityAshraf S. Youssef100% (2)
- Hydrogen Safety NFPADokument22 SeitenHydrogen Safety NFPArome_n21100% (1)
- ASTM E1417 Penetrant Testing - 9 PDFDokument11 SeitenASTM E1417 Penetrant Testing - 9 PDFbikaNoch keine Bewertungen
- Soft Tissue Augmentation Techniques in Implants Placed and Provisionalized Immediately. A Systematic Review.Dokument13 SeitenSoft Tissue Augmentation Techniques in Implants Placed and Provisionalized Immediately. A Systematic Review.andreita_loppNoch keine Bewertungen
- 380LC9S Performance PDFDokument21 Seiten380LC9S Performance PDFLuis Antonio Vega ParangueoNoch keine Bewertungen
- Longevity of Posterior Composite RestorationDokument15 SeitenLongevity of Posterior Composite Restorationvrana23Noch keine Bewertungen
- 8×8 LED Matrix MAX7219 With Scrolling Text & Android Control Via BluetoothDokument15 Seiten8×8 LED Matrix MAX7219 With Scrolling Text & Android Control Via BluetoothakashlogicNoch keine Bewertungen
- Darosarodolpho 2011Dokument9 SeitenDarosarodolpho 2011Rafaelly CubasNoch keine Bewertungen
- Longevity of Posterior Composite Restorations: Not Only A Matter of MaterialsDokument15 SeitenLongevity of Posterior Composite Restorations: Not Only A Matter of MaterialsKalpanaNoch keine Bewertungen
- Longevity of Posterior Composite RestoraDokument15 SeitenLongevity of Posterior Composite RestoraMelissa SierraNoch keine Bewertungen
- Full Arch Implant Supported Rehabilitations: A Prospective Study Comparing Porcelain Veneered Zirconia Frameworks To Monolithic ZirconiaDokument11 SeitenFull Arch Implant Supported Rehabilitations: A Prospective Study Comparing Porcelain Veneered Zirconia Frameworks To Monolithic ZirconiasnkidNoch keine Bewertungen
- Da Rosa Rodolpho 33 YearsDokument9 SeitenDa Rosa Rodolpho 33 YearsRafaelly CubasNoch keine Bewertungen
- Fixed Partial Dentures in An Up To 8-Year Follow-UpDokument8 SeitenFixed Partial Dentures in An Up To 8-Year Follow-Updaniel187951Noch keine Bewertungen
- Nanohybrid Versus Nano LL Composite in Class I CavitiesDokument5 SeitenNanohybrid Versus Nano LL Composite in Class I CavitiessonygabrielNoch keine Bewertungen
- Articol EPRDokument13 SeitenArticol EPRDiana TanasaNoch keine Bewertungen
- Darosarodolpho 2006Dokument9 SeitenDarosarodolpho 2006Rafaelly CubasNoch keine Bewertungen
- A Histopathologic Study On Pulp Response To Glass Ionomer Cements in Human TeethDokument8 SeitenA Histopathologic Study On Pulp Response To Glass Ionomer Cements in Human Teethnahm17Noch keine Bewertungen
- DirectCompositesversusIndirectCompositeInlays One YearResultsDokument11 SeitenDirectCompositesversusIndirectCompositeInlays One YearResultsAya Ibrahim YassinNoch keine Bewertungen
- Do Glass Ionomer Cements Prevent Caries On The Margins of Restaurations in Primary TeethDokument9 SeitenDo Glass Ionomer Cements Prevent Caries On The Margins of Restaurations in Primary TeethDoruNoch keine Bewertungen
- Articulo 8Dokument10 SeitenArticulo 8SofiaNoch keine Bewertungen
- Influence of Viscosity and Chemical Composition of Composite Resins in Non Carious Cervical Restorations 12 Month Randomized Clinical TrialDokument12 SeitenInfluence of Viscosity and Chemical Composition of Composite Resins in Non Carious Cervical Restorations 12 Month Randomized Clinical TrialŞtefania ZalăNoch keine Bewertungen
- Clinical Performance of Bulk-Fill and Conventional Resin Composite Restorations in Posterior Teeth: A Systematic Review and Meta-AnalysisDokument13 SeitenClinical Performance of Bulk-Fill and Conventional Resin Composite Restorations in Posterior Teeth: A Systematic Review and Meta-AnalysisNicolás SotoNoch keine Bewertungen
- Kunz Pvm. 2022.Dokument17 SeitenKunz Pvm. 2022.Nicolás SotoNoch keine Bewertungen
- Direct Resin Composite Restorations Versus Indirect Composite Inlays: One-Year ResultsDokument10 SeitenDirect Resin Composite Restorations Versus Indirect Composite Inlays: One-Year ResultsHari PriyaNoch keine Bewertungen
- Clinical Evaluation of Nanofilled Composite in Posterior TeethDokument9 SeitenClinical Evaluation of Nanofilled Composite in Posterior TeethsonygabrielNoch keine Bewertungen
- Daveiga 2016Dokument35 SeitenDaveiga 2016Andrei OanaNoch keine Bewertungen
- Long-Term Survival and Reasons For Failure in Direct Anterior Composite Restorations - A Systematic ReviewDokument10 SeitenLong-Term Survival and Reasons For Failure in Direct Anterior Composite Restorations - A Systematic ReviewArcelino FariasNoch keine Bewertungen
- Is Composite Repair Suitable For Anterior Restorations? A Long-Term Practice-Based Clinical StudyDokument10 SeitenIs Composite Repair Suitable For Anterior Restorations? A Long-Term Practice-Based Clinical StudyclaudiaNoch keine Bewertungen
- Longevity of Posterior Resin Composite Restorations in Adults - A Systematic ReviewDokument21 SeitenLongevity of Posterior Resin Composite Restorations in Adults - A Systematic ReviewCarla FloresNoch keine Bewertungen
- Three-Year Clinical Performance of Composite Restorations Placed by Undergraduate Dental StudentsDokument6 SeitenThree-Year Clinical Performance of Composite Restorations Placed by Undergraduate Dental StudentsFaiz Ahmad HamzahNoch keine Bewertungen
- Restorations in Primary Teeth: A Systematic Review On Survival and Reasons For FailuresDokument17 SeitenRestorations in Primary Teeth: A Systematic Review On Survival and Reasons For FailuresMel LlerenaNoch keine Bewertungen
- Selection of Dental Materials and Longevity of Replaced Restorations in Public Dental Health Clinics in Northern SwedenDokument6 SeitenSelection of Dental Materials and Longevity of Replaced Restorations in Public Dental Health Clinics in Northern SwedenClara CarneiroNoch keine Bewertungen
- Skupien 2016Dokument6 SeitenSkupien 2016valperlunNoch keine Bewertungen
- 66-Blinded Manuscript-66-1-10-20151003Dokument8 Seiten66-Blinded Manuscript-66-1-10-20151003ajengwidyapyahoo.comNoch keine Bewertungen
- 2 AutoresDokument3 Seiten2 AutoresCarlos FloriánNoch keine Bewertungen
- Laske 2016Dokument6 SeitenLaske 2016KaouterNoch keine Bewertungen
- 21 CoDokument26 Seiten21 CoSaad LiaqatNoch keine Bewertungen
- RostDokument56 SeitenRostandi boyNoch keine Bewertungen
- The Longevity of Restorations - A Literature Review: AcronymsDokument4 SeitenThe Longevity of Restorations - A Literature Review: AcronymsrintanfsNoch keine Bewertungen
- Clinical Trial Pulpotomy Biodentine Vs MtaDokument7 SeitenClinical Trial Pulpotomy Biodentine Vs MtagiselaNoch keine Bewertungen
- Longterm Survey All Ceramic Inlays Onlays Quintessnce 2020Dokument11 SeitenLongterm Survey All Ceramic Inlays Onlays Quintessnce 2020Raghu PratapNoch keine Bewertungen
- DirectResinCompositeRestorationsversusIndirectCompositeInlays One YearResultsDokument11 SeitenDirectResinCompositeRestorationsversusIndirectCompositeInlays One YearResultsSweetz Viena ParamitaNoch keine Bewertungen
- Consensus On Glass-Ionomer Cement Thresholds For Restorative IndicationsDokument8 SeitenConsensus On Glass-Ionomer Cement Thresholds For Restorative Indicationsviridiana perezNoch keine Bewertungen
- Direct Versus Indirect Inlayonlay Composite Restorations in Posterior Teeth. A Systematic Review and Meta-Analysis PDFDokument10 SeitenDirect Versus Indirect Inlayonlay Composite Restorations in Posterior Teeth. A Systematic Review and Meta-Analysis PDFMel LlerenaNoch keine Bewertungen
- NANO EN INDIRECTAS - PDFDokument7 SeitenNANO EN INDIRECTAS - PDFManuel Roberto Sarmiento LimasNoch keine Bewertungen
- INLAYDokument11 SeitenINLAYMira AnggrianiNoch keine Bewertungen
- PerioDokument6 SeitenPeriohusenahNoch keine Bewertungen
- Use of Fisiograft in Intrabony Defects-A Clinical and Radiological StudyDokument4 SeitenUse of Fisiograft in Intrabony Defects-A Clinical and Radiological StudymaxNoch keine Bewertungen
- Regenerative Endodontic Therapy in TheDokument14 SeitenRegenerative Endodontic Therapy in TheLouhanne LimaNoch keine Bewertungen
- 10 53424-Balikesirsbd 1062218-2209506Dokument7 Seiten10 53424-Balikesirsbd 1062218-2209506obenimNoch keine Bewertungen
- Implant-Supported Removable Partial Dentures in The Mandible A 3-16 Year Retrospective StudyDokument8 SeitenImplant-Supported Removable Partial Dentures in The Mandible A 3-16 Year Retrospective StudyMohammad Fadyl YunizarNoch keine Bewertungen
- Revisión Sistemática de Postes en OdontologíaDokument6 SeitenRevisión Sistemática de Postes en OdontologíaAxelJaraNoch keine Bewertungen
- Review Article: Ridge Preservation Procedures After Tooth Extractions: A Systematic ReviewDokument8 SeitenReview Article: Ridge Preservation Procedures After Tooth Extractions: A Systematic ReviewIka KusumawatiNoch keine Bewertungen
- Systematic Review of Lithium Disilicate MaterialsDokument9 SeitenSystematic Review of Lithium Disilicate Materialscarolina_indian100% (1)
- Analysis of Masticatory Cycle EfficiencyDokument4 SeitenAnalysis of Masticatory Cycle EfficiencyAndreeaSinNoch keine Bewertungen
- Jced 13 E935Dokument6 SeitenJced 13 E935Marwa Wagih ElboraeyNoch keine Bewertungen
- JIAP October 2011 - The Influence of Restorations and Prosthetic Crowns Finishing Lines On Inflammatory Levels After Non-Surgical Periodontal TherapyDokument8 SeitenJIAP October 2011 - The Influence of Restorations and Prosthetic Crowns Finishing Lines On Inflammatory Levels After Non-Surgical Periodontal TherapyMedstudNoch keine Bewertungen
- Trabajo A Presentar CBCT2Dokument6 SeitenTrabajo A Presentar CBCT2felipe martinezNoch keine Bewertungen
- IdilDikbas SWJDokument9 SeitenIdilDikbas SWJgerardo jimenezNoch keine Bewertungen
- Age of Restorations at Replacement in Permanent Teeth in General Dental PracticeDokument5 SeitenAge of Restorations at Replacement in Permanent Teeth in General Dental PracticehmsatNoch keine Bewertungen
- Jurnal Blok 2Dokument7 SeitenJurnal Blok 2Nifarea Anlila VesthiNoch keine Bewertungen
- Nobre 2016Dokument10 SeitenNobre 2016MonicaNoch keine Bewertungen
- Copenhagen 8 Yrlongevity JDent 2013Dokument11 SeitenCopenhagen 8 Yrlongevity JDent 2013Dan MPNoch keine Bewertungen
- Crestal Bone Level Around Tissue-Level Implants Restored With Platform Matching and Bone-Level ImplantsDokument9 SeitenCrestal Bone Level Around Tissue-Level Implants Restored With Platform Matching and Bone-Level Implantscd.brendasotofloresNoch keine Bewertungen
- Graftless Solutions for the Edentulous PatientVon EverandGraftless Solutions for the Edentulous PatientSaj JivrajNoch keine Bewertungen
- Salting-Out of Acetone From Water Basis of A New Solvent Extraction SystemDokument7 SeitenSalting-Out of Acetone From Water Basis of A New Solvent Extraction SystemAl-Kawthari As-Sunni100% (1)
- Emulsion-Stabilizing Effect of Gum From Acacia Senegal (L) WilldDokument5 SeitenEmulsion-Stabilizing Effect of Gum From Acacia Senegal (L) WilldAl-Kawthari As-SunniNoch keine Bewertungen
- Experiments and Modeling of Bubble Column Dehumidifier PerformanceDokument11 SeitenExperiments and Modeling of Bubble Column Dehumidifier PerformanceAl-Kawthari As-SunniNoch keine Bewertungen
- Heological Characterization of The Gel Point A New InterpretationDokument6 SeitenHeological Characterization of The Gel Point A New InterpretationAl-Kawthari As-SunniNoch keine Bewertungen
- Mathematical Functions For The Representation of Chromatographic PeaksDokument30 SeitenMathematical Functions For The Representation of Chromatographic PeaksAl-Kawthari As-SunniNoch keine Bewertungen
- InsulinDokument6 SeitenInsulinJorelle-Nickolai RodriguezNoch keine Bewertungen
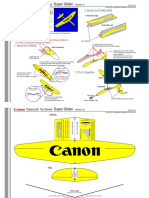
- Planeur Tres Simple PDFDokument3 SeitenPlaneur Tres Simple PDFAhmedNoch keine Bewertungen
- Modeling and Control of Side Face Beam Cracking - FroschDokument10 SeitenModeling and Control of Side Face Beam Cracking - FroschphamminhquangNoch keine Bewertungen
- Paradox Pir 476 Dg55 Dg55c Dg65 Dg65c Dg75 Dg75c 476 476pet Atm EtlDokument1 SeiteParadox Pir 476 Dg55 Dg55c Dg65 Dg65c Dg75 Dg75c 476 476pet Atm EtlTech StarNoch keine Bewertungen
- Ee BD ManualDokument37 SeitenEe BD Manualsergey62Noch keine Bewertungen
- Cryogenic and Its ApplicationDokument11 SeitenCryogenic and Its ApplicationBhoomika MansharamaniNoch keine Bewertungen
- Hyundai Heavy Industries - Gas Insulated SwitchgearDokument25 SeitenHyundai Heavy Industries - Gas Insulated SwitchgearbadbenzationNoch keine Bewertungen
- L3 - Hardening Soil Models in PlaxisDokument33 SeitenL3 - Hardening Soil Models in PlaxisOng Tai BoonNoch keine Bewertungen
- SuperOrca ManualDokument22 SeitenSuperOrca Manualarm usaNoch keine Bewertungen
- 1188CK ExampleDokument2 Seiten1188CK ExampleYurii ChinovNoch keine Bewertungen
- Subitec Info Industrial CultivationDokument4 SeitenSubitec Info Industrial CultivationUsamah ZakiNoch keine Bewertungen
- IQ RF MappingDokument14 SeitenIQ RF Mappingsatcom_77Noch keine Bewertungen
- CDMA APPLICATION FOR Child Name Inclusion-Before 1 Year PDFDokument2 SeitenCDMA APPLICATION FOR Child Name Inclusion-Before 1 Year PDFAnonymous C0pl6hNoch keine Bewertungen
- Ionic Equations & Redox ReactionsDokument6 SeitenIonic Equations & Redox ReactionsAyaanNashidNoch keine Bewertungen
- Enemy Territory - Quake Wars - ManualDokument22 SeitenEnemy Territory - Quake Wars - ManualM_MolliNoch keine Bewertungen
- Assimilable Organic Carbon Formation During Ultraviolet - Hydrogen Peroxide Advanced Oxidation Treatment of Surface WaterDokument207 SeitenAssimilable Organic Carbon Formation During Ultraviolet - Hydrogen Peroxide Advanced Oxidation Treatment of Surface WaterMonicaRossetimNoch keine Bewertungen
- Wind Loads - IS 875 - Where Does Our Code of Practice StandDokument11 SeitenWind Loads - IS 875 - Where Does Our Code of Practice StandRavi Kiran NandyalaNoch keine Bewertungen
- TTO-ST-0-SPC-05100 - Structural Steel SpecificationDokument18 SeitenTTO-ST-0-SPC-05100 - Structural Steel Specificationsara saravananNoch keine Bewertungen
- Data Sheet For Toys TestDokument2 SeitenData Sheet For Toys TestAnonymous TYGiADNoch keine Bewertungen
- Catalogo GIACOMINIDokument45 SeitenCatalogo GIACOMINIIsrael Silva Hgo.Noch keine Bewertungen
- Column Marking For G+4 Hostel Building: All Dimensions Are in MeterDokument1 SeiteColumn Marking For G+4 Hostel Building: All Dimensions Are in Metergowtham gowdaNoch keine Bewertungen
- Technician 1956 05Dokument118 SeitenTechnician 1956 05Harish sathelliNoch keine Bewertungen
- Bricks ComparisonDokument13 SeitenBricks ComparisonMd. Numan HossainNoch keine Bewertungen