Das könnte Ihnen auch gefallen
- PNF PatternsDokument19 SeitenPNF PatternsDany VirgilNoch keine Bewertungen
- Sexual Disorders ParaphiliaDokument32 SeitenSexual Disorders Paraphiliaitsmeaya0% (1)
- Post Abortion CareDokument35 SeitenPost Abortion CareNatukunda DianahNoch keine Bewertungen
- Drug Development: FDA's Definition of A New DrugDokument11 SeitenDrug Development: FDA's Definition of A New DrugSophie MendezNoch keine Bewertungen
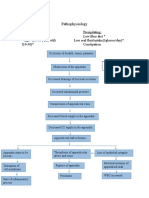
- Appendicitis PathophysiologyDokument2 SeitenAppendicitis PathophysiologyitsmeayaNoch keine Bewertungen
- Acute Pancreatitis: Causes, Symptoms, Diagnosis & TreatmentDokument3 SeitenAcute Pancreatitis: Causes, Symptoms, Diagnosis & TreatmentitsmeayaNoch keine Bewertungen
- War Wounds: Basic Surgical Management: The Principles and Practice of The Surgical Management of Wounds Produced by Missiles or ExplosionsDokument48 SeitenWar Wounds: Basic Surgical Management: The Principles and Practice of The Surgical Management of Wounds Produced by Missiles or ExplosionsInternational Committee of the Red Cross86% (7)
- Coping With Stress Senior HighDokument23 SeitenCoping With Stress Senior HighJulienne Rose Penaranda Saballa100% (1)
- Dimenhydrinate PDFDokument2 SeitenDimenhydrinate PDFWindy SengiNoch keine Bewertungen
- Pediatrics Pediatrics Pediatrics Pediatrics Pediatrics: Pediatrics Pediatrics Pediatrics Pediatrics PediatricsDokument2 SeitenPediatrics Pediatrics Pediatrics Pediatrics Pediatrics: Pediatrics Pediatrics Pediatrics Pediatrics PediatricsBobet Reña100% (2)
- DRUG STUDY Allopurinol (Purinase)Dokument2 SeitenDRUG STUDY Allopurinol (Purinase)DennMarkTaponNoch keine Bewertungen
- Mental Status ExaminationDokument4 SeitenMental Status Examinationitsmeaya100% (3)
- DRUG STUDY EpinephrineDokument2 SeitenDRUG STUDY EpinephrineCarlo Francisco D. Canto78% (9)
- Drug StudyDokument9 SeitenDrug Studykcbabee0333% (3)
- Drug Study of Ceftriaxone & RowatinexDokument5 SeitenDrug Study of Ceftriaxone & RowatinexLorina Lynne ApelacioNoch keine Bewertungen
- Drug StudyDokument9 SeitenDrug StudyJonica CamposNoch keine Bewertungen
- San Pedro Hospital of Davao City, Inc.: Nurses' NotesDokument2 SeitenSan Pedro Hospital of Davao City, Inc.: Nurses' NotesSophia Jay LaurieNoch keine Bewertungen
- NCP - FatigueDokument3 SeitenNCP - Fatigueitsmeaya100% (1)
- Nifedipine and Prednisone Drug StudyDokument5 SeitenNifedipine and Prednisone Drug StudyAllyne GavinoNoch keine Bewertungen
- Acceptance of Dying A Discourse Analysis of Palliative Care LiteratureDokument8 SeitenAcceptance of Dying A Discourse Analysis of Palliative Care LiteratureMauricio MartinezNoch keine Bewertungen
- KetorolacDokument5 SeitenKetorolacMichelle Ann P. NacuaNoch keine Bewertungen
- Drug StudyDokument13 SeitenDrug StudyAldrin Ian Oraza AlpeNoch keine Bewertungen
- Drug study cilostazol intermittent claudicationDokument2 SeitenDrug study cilostazol intermittent claudicationart_mutantNoch keine Bewertungen
- Amoxicillin Nursing ConsiderationsDokument3 SeitenAmoxicillin Nursing ConsiderationsNico DonatoNoch keine Bewertungen
- Drug mechanism indication contraindication side effects nursingDokument1 SeiteDrug mechanism indication contraindication side effects nursinghahahahaaaaaaaNoch keine Bewertungen
- DioxelDokument1 SeiteDioxelJosselle Sempio CalientaNoch keine Bewertungen
- DuphalacDokument2 SeitenDuphalacianecunarNoch keine Bewertungen
- Drug AnalysisDokument8 SeitenDrug AnalysisJonie Vince SañosaNoch keine Bewertungen
- COLCHICINE pptx1800128929Dokument15 SeitenCOLCHICINE pptx1800128929April Mergelle LapuzNoch keine Bewertungen
- Drug Study: Name of Drug Action Indication Adverse Effect Nursing ResponsibilityDokument4 SeitenDrug Study: Name of Drug Action Indication Adverse Effect Nursing ResponsibilityBel CortezNoch keine Bewertungen
- Drug Study Ko ToDokument4 SeitenDrug Study Ko ToGian Carlo FernandezNoch keine Bewertungen
- 66 Drug AnaDokument3 Seiten66 Drug AnaAlexa RoqueNoch keine Bewertungen
- Biperiden Generic and Brand Names, Uses, Side EffectsDokument1 SeiteBiperiden Generic and Brand Names, Uses, Side EffectsMFQ.RN100% (2)
- DS (Fenofibrate)Dokument5 SeitenDS (Fenofibrate)Mary April MendezNoch keine Bewertungen
- DRUGS Study OrigDokument17 SeitenDRUGS Study OrigKiersten Karen Policarpio Verina100% (1)
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDokument2 SeitenAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationAbigail BascoNoch keine Bewertungen
- Cefazolin Sodium AncefDokument1 SeiteCefazolin Sodium AncefKristi WrayNoch keine Bewertungen
- Drug Study FinalDokument5 SeitenDrug Study FinalJackie Ann Marie DapatNoch keine Bewertungen
- Discharge PlanDokument4 SeitenDischarge PlanVillanueva NiñaNoch keine Bewertungen
- Drug Study Cushing's SyndromeDokument5 SeitenDrug Study Cushing's SyndromeSelena MarieNoch keine Bewertungen
- Drug StudyDokument8 SeitenDrug StudyRizzi DeveraNoch keine Bewertungen
- Atropine SulfateDokument1 SeiteAtropine SulfateTrishaaMayolNoch keine Bewertungen
- Chromium Picolinate Drug StudyDokument1 SeiteChromium Picolinate Drug StudyjoellaNoch keine Bewertungen
- DS (Calcium + Vit. D)Dokument6 SeitenDS (Calcium + Vit. D)Mary April MendezNoch keine Bewertungen
- NafarinDokument2 SeitenNafarinianecunar100% (2)
- Metoclopramide Drug Study: Uses, Side Effects, Nursing ConsiderationsDokument2 SeitenMetoclopramide Drug Study: Uses, Side Effects, Nursing ConsiderationsJohn Paolo Tamayo OrioNoch keine Bewertungen
- DRUG-STUDY - BALLON, Karlo CDokument6 SeitenDRUG-STUDY - BALLON, Karlo CMelinda Cariño BallonNoch keine Bewertungen
- Drug Study Stugeron and Kalium DuruleDokument1 SeiteDrug Study Stugeron and Kalium DuruleawesomedawnNoch keine Bewertungen
- Assessing and Treating Post-Operative HypothermiaDokument2 SeitenAssessing and Treating Post-Operative HypothermiaJayrelle D. SafranNoch keine Bewertungen
- CefoperazoneDokument3 SeitenCefoperazoneBaim FarmaNoch keine Bewertungen
- Drug StudyDokument10 SeitenDrug Studyjho_26100% (2)
- AtroventDokument2 SeitenAtroventKatie McPeekNoch keine Bewertungen
- Drug Study - AmlodipineDokument1 SeiteDrug Study - AmlodipineDanielle Marie SamblacenoNoch keine Bewertungen
- Apixaban 5 PDFDokument2 SeitenApixaban 5 PDFWanie Al-basriNoch keine Bewertungen
- Drug StudyDokument5 SeitenDrug StudyBridgette ArañesNoch keine Bewertungen
- ItoprideDokument2 SeitenItoprideLesValenzuelaNoch keine Bewertungen
- LacipilDokument2 SeitenLacipilianecunarNoch keine Bewertungen
- Chn-Herbal MedicineDokument5 SeitenChn-Herbal MedicineBSN 1-N CASTRO, RicciNoch keine Bewertungen
- Discharge Plan CapDokument3 SeitenDischarge Plan Capalexander abasNoch keine Bewertungen
- Drug StudiesDokument16 SeitenDrug Studiesvitcloud23100% (2)
- Ertapenem (Invanz)Dokument1 SeiteErtapenem (Invanz)Adrianne BazoNoch keine Bewertungen
- D50WDokument1 SeiteD50WElizalde Husband100% (1)
- Solu-Cortef (Hydrocortisone)Dokument3 SeitenSolu-Cortef (Hydrocortisone)E100% (2)
- Example of Drug StudyDokument2 SeitenExample of Drug Studydonna mae junioNoch keine Bewertungen
- Drug AnalysisDokument3 SeitenDrug AnalysisAbby BorabienNoch keine Bewertungen
- Metronidazole 500mg/tab 1 Tab 3xadayDokument4 SeitenMetronidazole 500mg/tab 1 Tab 3xadayCrisyl LipawenNoch keine Bewertungen
- Assessment Diagnosis Planning Intervention Rationale EvaluationDokument4 SeitenAssessment Diagnosis Planning Intervention Rationale EvaluationJhoizel VenusNoch keine Bewertungen
- Drug StudyDokument4 SeitenDrug StudyXio PauNoch keine Bewertungen
- Verapamil HCLDokument3 SeitenVerapamil HCLMae Ann Bueno CastillonNoch keine Bewertungen
- Cefuroxime Anti-Bacterial CephalosporinDokument9 SeitenCefuroxime Anti-Bacterial CephalosporinDustin JohnNoch keine Bewertungen
- GENERIC NAME: Ranitidine BRAND NAME: Zantac CLASSIFICATION Therapeutic: Anti-Ulcer AgentsDokument4 SeitenGENERIC NAME: Ranitidine BRAND NAME: Zantac CLASSIFICATION Therapeutic: Anti-Ulcer Agentsehnna50% (2)
- Drug Name Mechanism of Action Indication Contraindication Drug'S Effect Nsg. ConsiderationDokument2 SeitenDrug Name Mechanism of Action Indication Contraindication Drug'S Effect Nsg. ConsiderationKatrina PonceNoch keine Bewertungen
- Gastrointestinal System: Antihistamine Half-Life: Onset: Peaks: DurationDokument3 SeitenGastrointestinal System: Antihistamine Half-Life: Onset: Peaks: DurationsyerlyNoch keine Bewertungen
- Acetylcysteine, Phenytoin, Gentamicin, Captopril, Pilocarpine Nursing ResponsibilitiesDokument7 SeitenAcetylcysteine, Phenytoin, Gentamicin, Captopril, Pilocarpine Nursing ResponsibilitieseyesidphNoch keine Bewertungen
- Promoting Activity Tolerance in a Patient with CoughDokument3 SeitenPromoting Activity Tolerance in a Patient with CoughitsmeayaNoch keine Bewertungen
- Patient Classification Systems: A GuideDokument69 SeitenPatient Classification Systems: A GuideitsmeayaNoch keine Bewertungen
- Impact of Philippines Pantawid Pamilyang Pilipino ProgramDokument2 SeitenImpact of Philippines Pantawid Pamilyang Pilipino Programitsmeaya0% (1)
- Acute GlomerulonephritisDokument4 SeitenAcute GlomerulonephritisitsmeayaNoch keine Bewertungen
- Drug Study FormatDokument1 SeiteDrug Study FormatitsmeayaNoch keine Bewertungen
- Kwashiorkor and MarasmusDokument2 SeitenKwashiorkor and Marasmusitsmeaya100% (1)
- Nursing Care Plan General Objective: To Promote Safety Through Prevention of The Spread of InfectionDokument3 SeitenNursing Care Plan General Objective: To Promote Safety Through Prevention of The Spread of InfectionitsmeayaNoch keine Bewertungen
- Food Safety ChecklistDokument2 SeitenFood Safety ChecklistitsmeayaNoch keine Bewertungen
- Benner's TheoryDokument15 SeitenBenner's TheoryitsmeayaNoch keine Bewertungen
- AnorexicDokument15 SeitenAnorexicitsmeayaNoch keine Bewertungen
- AnorexicDokument15 SeitenAnorexicitsmeayaNoch keine Bewertungen
- General Appearance: The: Patient Was On Semi Fowler's Position During Assessment and Body Weakness Was NotedDokument9 SeitenGeneral Appearance: The: Patient Was On Semi Fowler's Position During Assessment and Body Weakness Was NoteditsmeayaNoch keine Bewertungen
- External HemorrhoidsDokument61 SeitenExternal HemorrhoidsitsmeayaNoch keine Bewertungen
- Cues Problem Physiologic Behavioral: Date Identified: July 19, 2016 Subjective CuesDokument2 SeitenCues Problem Physiologic Behavioral: Date Identified: July 19, 2016 Subjective CuesitsmeayaNoch keine Bewertungen
- Benner's TheoryDokument15 SeitenBenner's TheoryitsmeayaNoch keine Bewertungen
- Red Blood CellsDokument3 SeitenRed Blood CellsitsmeayaNoch keine Bewertungen
- Subjective Cues:: IndependentDokument4 SeitenSubjective Cues:: IndependentitsmeayaNoch keine Bewertungen
- Or ObjectivesDokument1 SeiteOr ObjectivesitsmeayaNoch keine Bewertungen
- Chole Lithia SisDokument4 SeitenChole Lithia SisitsmeayaNoch keine Bewertungen
- Generic Name Brand Name Drug Classification Mechanism of Action Indications Adverse Reaction Nursing ResponsibilitiesDokument1 SeiteGeneric Name Brand Name Drug Classification Mechanism of Action Indications Adverse Reaction Nursing ResponsibilitiesitsmeayaNoch keine Bewertungen
- Staff Nursing ResponsibilitiesDokument3 SeitenStaff Nursing ResponsibilitiesitsmeayaNoch keine Bewertungen
- Staff Nursing ResponsibilitiesDokument3 SeitenStaff Nursing ResponsibilitiesitsmeayaNoch keine Bewertungen
- IntroductionDokument1 SeiteIntroductionitsmeayaNoch keine Bewertungen
- GNFDokument2 SeitenGNFitsmeayaNoch keine Bewertungen
- Skin Is The Largest Organ of The Human BodyDokument4 SeitenSkin Is The Largest Organ of The Human BodyitsmeayaNoch keine Bewertungen
- Capstone PosterDokument1 SeiteCapstone Posterapi-273438577Noch keine Bewertungen
- CLOZE TEST Discovery Could Ease Blood ShortageDokument2 SeitenCLOZE TEST Discovery Could Ease Blood ShortageKarsan Ayaz MaierNoch keine Bewertungen
- ICNCDRS Blindness Registry FormDokument4 SeitenICNCDRS Blindness Registry FormAprilAngeliRobleNoch keine Bewertungen
- Medical History QuestionnaireDokument3 SeitenMedical History QuestionnaireSachitra Nirman MalwatteNoch keine Bewertungen
- Causes of Foamy UrineDokument12 SeitenCauses of Foamy UrineAishwariyaaAngelinaStephenNoch keine Bewertungen
- Literature Review For Specimen Labeling and Blood BankDokument3 SeitenLiterature Review For Specimen Labeling and Blood Bankapi-236445988Noch keine Bewertungen
- Adult Grip Strength Norms For The Baseline Digital DynamometerDokument25 SeitenAdult Grip Strength Norms For The Baseline Digital DynamometerOmar Escalante DíazNoch keine Bewertungen
- The Shouldice Repair: Robert Bendavid, MDDokument14 SeitenThe Shouldice Repair: Robert Bendavid, MDmarquete72Noch keine Bewertungen
- Basic Airway ManagementDokument98 SeitenBasic Airway ManagementRani Salsabilah100% (1)
- Management of Head InjuryDokument27 SeitenManagement of Head InjuryrosybashNoch keine Bewertungen
- Parotid Tumors and Other Salivary Gland TumorsDokument41 SeitenParotid Tumors and Other Salivary Gland Tumorsdrhiwaomer100% (9)
- Dr. Steven Corwin LetterDokument2 SeitenDr. Steven Corwin LetterJonathan LaMantiaNoch keine Bewertungen
- Gastritis PDFDokument6 SeitenGastritis PDFsrimardiahkusumaNoch keine Bewertungen
- Jurnal Pendukung 2Dokument13 SeitenJurnal Pendukung 2Eko PrasNoch keine Bewertungen
- Disclosures: Kori Dewing, DNP, ARNP Virginia Mason Medical Center October 29, 2013Dokument3 SeitenDisclosures: Kori Dewing, DNP, ARNP Virginia Mason Medical Center October 29, 2013Alexander Diaz ZuletaNoch keine Bewertungen
- Guillian-Barre Syndrome: Renalyn Galache Gladys Gegare BSN-3BDokument18 SeitenGuillian-Barre Syndrome: Renalyn Galache Gladys Gegare BSN-3BGLadys GegareNoch keine Bewertungen
- Preoperative Diagnosis of A Third Root Canal in First and Second Maxillary Premolars A Challenge For The ClinicianDokument7 SeitenPreoperative Diagnosis of A Third Root Canal in First and Second Maxillary Premolars A Challenge For The ClinicianS S Saad SaadNoch keine Bewertungen
- TriageDokument42 SeitenTriageNic JiNoch keine Bewertungen
- Shock Resident LectureDokument38 SeitenShock Resident Lecturepapermate9293Noch keine Bewertungen
- Lecture 4 Medical Terminology PDFDokument38 SeitenLecture 4 Medical Terminology PDFAhmed KhaledNoch keine Bewertungen
- Psychiatry IntroductionDokument26 SeitenPsychiatry IntroductionMunir AhmedNoch keine Bewertungen