Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Brosur Penyuluhan Gizi Anak SekolahDokument2 SeitenBrosur Penyuluhan Gizi Anak SekolahTia AriantiNoch keine Bewertungen
- Jurnal 1Dokument13 SeitenJurnal 1Tia AriantiNoch keine Bewertungen
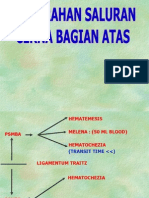
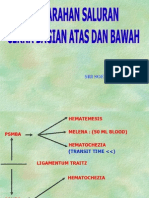
- Perdarahan Saluran Cerna Atas Dan BawahDokument24 SeitenPerdarahan Saluran Cerna Atas Dan BawahTia AriantiNoch keine Bewertungen
- Penyakit Jantung HipertensiDokument24 SeitenPenyakit Jantung HipertensiTia AriantiNoch keine Bewertungen
- Soal Ujian EkgDokument12 SeitenSoal Ujian EkgTia AriantiNoch keine Bewertungen
- Fatty Liver - HandoutDokument31 SeitenFatty Liver - HandoutTia AriantiNoch keine Bewertungen
- Chapter 9 Urinary System: Lesson 1Dokument23 SeitenChapter 9 Urinary System: Lesson 1Tia AriantiNoch keine Bewertungen
- Congestive Heart Failure CHF: Nik Nikam, M.DDokument94 SeitenCongestive Heart Failure CHF: Nik Nikam, M.DTia AriantiNoch keine Bewertungen
- Perdarahan Saluran Cerna Atas Dan BawahDokument34 SeitenPerdarahan Saluran Cerna Atas Dan BawahTia AriantiNoch keine Bewertungen
- Art and Science of UrinalysisDokument31 SeitenArt and Science of UrinalysisTia AriantiNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- P5vs-Module For Doctors 2Dokument70 SeitenP5vs-Module For Doctors 2asraf amirullahNoch keine Bewertungen
- Critical Thinking Case Study PharmaDokument2 SeitenCritical Thinking Case Study Pharmakimberly magsipocNoch keine Bewertungen
- Case Study Nursing SampleDokument9 SeitenCase Study Nursing SampleChloie Marie Rosalejos100% (1)
- Impaired Skin Integrity Related To Excess Fluids Volume As Evidenced by Swelling of The Lower ExtremitiesDokument2 SeitenImpaired Skin Integrity Related To Excess Fluids Volume As Evidenced by Swelling of The Lower ExtremitiesLevin MenpinNoch keine Bewertungen
- Early Warning SystemsDokument7 SeitenEarly Warning SystemsJamalNoch keine Bewertungen
- Pediatric Diagnosis PedDokument153 SeitenPediatric Diagnosis PedIceNoch keine Bewertungen
- Handout Checklist For Student AssistDokument9 SeitenHandout Checklist For Student AssistPrecious SorianoNoch keine Bewertungen
- Critikon Dinamap Compact - Service Manual 1 PDFDokument75 SeitenCritikon Dinamap Compact - Service Manual 1 PDFAyaovi JorlauNoch keine Bewertungen
- Lesson Five: Problem List, Vital Signs, Immunizations, Progress NoteDokument5 SeitenLesson Five: Problem List, Vital Signs, Immunizations, Progress NoteKayOBandz BabbiiiNoch keine Bewertungen
- Performance Checklist CPRDokument2 SeitenPerformance Checklist CPRMhel MGNoch keine Bewertungen
- SRNA Orientation ChecklistDokument40 SeitenSRNA Orientation Checklistihtisham1Noch keine Bewertungen
- Nursing Care Plan For Doppler Scan and Stress TestingDokument10 SeitenNursing Care Plan For Doppler Scan and Stress TestingAmy Rose AbuevaNoch keine Bewertungen
- Stan Checketts DocumentationDokument2 SeitenStan Checketts Documentationnikdolly50% (4)
- Final Exam Case StudyDokument6 SeitenFinal Exam Case StudyLoucil Ursula AranasNoch keine Bewertungen
- Vital Signs TakingDokument27 SeitenVital Signs TakingJames Paulo AbandoNoch keine Bewertungen
- Breast CancerDokument53 SeitenBreast CancerJCneriNoch keine Bewertungen
- Is This Patient HypovolemicDokument8 SeitenIs This Patient HypovolemicNicholasNoch keine Bewertungen
- Prittie-2006-Journal of Veterinary Emergency and Critical CareDokument11 SeitenPrittie-2006-Journal of Veterinary Emergency and Critical Carejose fdoNoch keine Bewertungen
- Terapi Bekam Dalam Menurunkan Intensitas Dismenore Dan Tanda-Tanda Vital (Nadi Dan Tekanan Darah)Dokument8 SeitenTerapi Bekam Dalam Menurunkan Intensitas Dismenore Dan Tanda-Tanda Vital (Nadi Dan Tekanan Darah)Milkha AmaliaNoch keine Bewertungen
- NPS ExamDokument21 SeitenNPS ExamJasmine JarapNoch keine Bewertungen
- Nursing 2Dokument50 SeitenNursing 2Rn nadeenNoch keine Bewertungen
- CVD Case StudyDokument76 SeitenCVD Case StudyThomas joshua QuiñonesNoch keine Bewertungen
- CBLM Core 1Dokument81 SeitenCBLM Core 1Jasper Carl David100% (1)
- Group Fdar Hemophilia ADokument2 SeitenGroup Fdar Hemophilia AMika SaldañaNoch keine Bewertungen
- Nephrotic Syndrome Case PresentationDokument22 SeitenNephrotic Syndrome Case PresentationmadhusreejyothinagaramvNoch keine Bewertungen
- G1P0, Placenta Previa: Discharge Plan DietDokument7 SeitenG1P0, Placenta Previa: Discharge Plan DietRap De la CruzNoch keine Bewertungen
- Nursing Care PlanDokument3 SeitenNursing Care PlanCrystelle MonaresNoch keine Bewertungen
- Vital Signs 2024Dokument50 SeitenVital Signs 2024gntawfeqNoch keine Bewertungen
- NUR 102 - Fundamentals of Nursing POIDokument22 SeitenNUR 102 - Fundamentals of Nursing POIDefprimalNoch keine Bewertungen
- NCPDokument2 SeitenNCPJonna Mae TurquezaNoch keine Bewertungen