Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Vaccination Myths - A. G. PhillipsDokument11 SeitenVaccination Myths - A. G. PhillipsBrendan D. MurphyNoch keine Bewertungen
- PertussisDokument21 SeitenPertussisjco jac100% (1)
- Medical Form For Grade 7 12Dokument3 SeitenMedical Form For Grade 7 12Deonna Angeline100% (1)
- Normal NewbornDokument30 SeitenNormal NewbornLekshmi Manu100% (3)
- Chapter 1Dokument52 SeitenChapter 1marialourdes2489100% (15)
- Communicable Disease NursingDokument7 SeitenCommunicable Disease NursingNimrodNoch keine Bewertungen
- Tetanus Recommendations TRS 980 Annex 5 PDFDokument63 SeitenTetanus Recommendations TRS 980 Annex 5 PDFIchaickenNoch keine Bewertungen
- Cigna'S Preventive Health Coverage: A Guide ToDokument12 SeitenCigna'S Preventive Health Coverage: A Guide TomcrphNoch keine Bewertungen
- CHN1Dokument898 SeitenCHN1Mraclne Olaño0% (1)
- Jawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthDokument18 SeitenJawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthIvan OliveiraNoch keine Bewertungen
- Systemic Peads Notes Growth Development Psychiatry NutritionDokument26 SeitenSystemic Peads Notes Growth Development Psychiatry NutritionusamaNoch keine Bewertungen
- Community Health NursingDokument516 SeitenCommunity Health NursingFabby Vitacion Tan75% (4)
- NSW Immunisation ScheduleDokument1 SeiteNSW Immunisation ScheduleKristinaNoch keine Bewertungen
- Immunisation 2013 PDFDokument1 SeiteImmunisation 2013 PDFjuniorebindaNoch keine Bewertungen
- CMR Matoo and Cherry 2005Dokument58 SeitenCMR Matoo and Cherry 2005fznmominNoch keine Bewertungen
- Alberta TetanusDokument7 SeitenAlberta TetanusranggaNoch keine Bewertungen
- Wil Document Requirements Passport 1Dokument3 SeitenWil Document Requirements Passport 1api-283084320Noch keine Bewertungen
- BP2012 IndexDokument68 SeitenBP2012 IndexAsif AhmedNoch keine Bewertungen
- SRB DepDokument1.302 SeitenSRB DepCrystal TsaiNoch keine Bewertungen
- FINAL EXAM REVIEW CHN 1Dokument43 SeitenFINAL EXAM REVIEW CHN 1Maria Luz S. RulonaNoch keine Bewertungen
- Report of The Inter-Departmental Group On Mother and Baby Homes-June 2014Dokument37 SeitenReport of The Inter-Departmental Group On Mother and Baby Homes-June 2014Rick ThomaNoch keine Bewertungen
- Vaccine BookDokument37 SeitenVaccine Bookrafael alvarizNoch keine Bewertungen
- Staying Healthy in Childcare - Gov Handbook - 4th EditionDokument138 SeitenStaying Healthy in Childcare - Gov Handbook - 4th EditionSarah Williamson PhippsNoch keine Bewertungen
- Acronyms & AbbreviationsDokument70 SeitenAcronyms & Abbreviationsravip3366Noch keine Bewertungen
- TetanusDokument18 SeitenTetanusMichael EatonNoch keine Bewertungen
- Epi PediaDokument1 SeiteEpi Pediag3nj1Noch keine Bewertungen
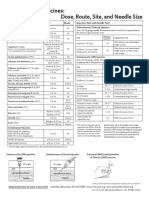
- Injection Site and Needle Size Vaccine Dose RouteDokument1 SeiteInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaNoch keine Bewertungen
- Answers & Solutions: For For For For For AIPMT-2015Dokument28 SeitenAnswers & Solutions: For For For For For AIPMT-2015Souradeep DebNoch keine Bewertungen
- Page numbers in bold relate to monograph titlesDokument66 SeitenPage numbers in bold relate to monograph titlesMahesh_ChokshiNoch keine Bewertungen
- Thorpe 2015Dokument15 SeitenThorpe 2015Olivia HariyantoNoch keine Bewertungen