Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Maniac MansionDokument5 SeitenManiac MansionRias SahulNoch keine Bewertungen
- Guide Iso50001 Checklist PDFDokument16 SeitenGuide Iso50001 Checklist PDFRias SahulNoch keine Bewertungen
- UntitledDokument385 SeitenUntitledNiaz RNoch keine Bewertungen
- Administer WSH Policy - Written Assignment 1Dokument5 SeitenAdminister WSH Policy - Written Assignment 1Rias Sahul58% (19)
- SMB013 Risk Assessment Use Storage and Disposal of Flammable LiquidsDokument6 SeitenSMB013 Risk Assessment Use Storage and Disposal of Flammable LiquidsRias SahulNoch keine Bewertungen
- Strongly Disagree Disagree Neutral 1,275 1,275 1,275 3,879 6,464 7,757 0 Slightly Agree Moderat Ely Agree Highly Agree Not Applicabl EtomeDokument4 SeitenStrongly Disagree Disagree Neutral 1,275 1,275 1,275 3,879 6,464 7,757 0 Slightly Agree Moderat Ely Agree Highly Agree Not Applicabl EtomeRias Sahul0% (1)
- Norman Lee - ActsysDokument27 SeitenNorman Lee - ActsysRias SahulNoch keine Bewertungen
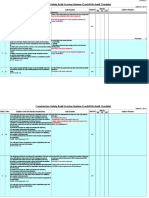
- Consass ChecklistDokument61 SeitenConsass ChecklistRias SahulNoch keine Bewertungen
- Consass ChecklistDokument61 SeitenConsass ChecklistRias SahulNoch keine Bewertungen
- Safety Training Session Evaluation FormDokument1 SeiteSafety Training Session Evaluation FormRias SahulNoch keine Bewertungen
- 5.5.1 Performance Measurement and MonitoringDokument2 Seiten5.5.1 Performance Measurement and MonitoringRias SahulNoch keine Bewertungen
- Workplace Safety and Health Framework Development and ImplementationDokument3 SeitenWorkplace Safety and Health Framework Development and ImplementationRias SahulNoch keine Bewertungen
- Delgato Asking The Right QuestionsDokument2 SeitenDelgato Asking The Right QuestionsRias SahulNoch keine Bewertungen
- 2015 CN3132 II Lecture 01 Mass Transfer ModelsDokument20 Seiten2015 CN3132 II Lecture 01 Mass Transfer ModelsRias SahulNoch keine Bewertungen
- Final Report TemplateDokument13 SeitenFinal Report TemplateRias SahulNoch keine Bewertungen
- CN4250 - Chapter 0 - IntroductionDokument1 SeiteCN4250 - Chapter 0 - IntroductionRias SahulNoch keine Bewertungen
- ScriptDokument21 SeitenScriptRias SahulNoch keine Bewertungen
- Design Project Statement - AY 2016-17Dokument2 SeitenDesign Project Statement - AY 2016-17Rias SahulNoch keine Bewertungen
- Tutorial 3 QN 3Dokument2 SeitenTutorial 3 QN 3Rias SahulNoch keine Bewertungen
- Lab 1 Data Sheet: System 1 (Naoh + HCL)Dokument4 SeitenLab 1 Data Sheet: System 1 (Naoh + HCL)Rias SahulNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- OTN HierarchyDokument6 SeitenOTN Hierarchyiss155Noch keine Bewertungen
- Muhammed Abrar - Salesforce DeveloperDokument1 SeiteMuhammed Abrar - Salesforce DeveloperKarthik KingNoch keine Bewertungen
- Cut Off Points Private. Ay 2020-2021 AdmissionsDokument6 SeitenCut Off Points Private. Ay 2020-2021 AdmissionsRonnie AtuhaireNoch keine Bewertungen
- Banks Betting Big On Big Data and Real-Time Customer InsightDokument5 SeitenBanks Betting Big On Big Data and Real-Time Customer InsightShahid_ONNoch keine Bewertungen
- Mc2550 Tech GuideDokument42 SeitenMc2550 Tech Guidecynneath4045Noch keine Bewertungen
- Resistron: Operating InstructionsDokument51 SeitenResistron: Operating Instructions16_45_2013_gabri0% (1)
- Documenting Software Architectures: Views and Beyond: June 2002Dokument3 SeitenDocumenting Software Architectures: Views and Beyond: June 2002Ioan AdascaliteiNoch keine Bewertungen
- Datasheet - HK S29al016j70tfi020 6599589Dokument58 SeitenDatasheet - HK S29al016j70tfi020 6599589SAABNoch keine Bewertungen
- Grounding Considerations For Large kVA Pad-Mount TransformersDokument4 SeitenGrounding Considerations For Large kVA Pad-Mount TransformersRuwan DeegayuNoch keine Bewertungen
- Blockchain BasicsDokument17 SeitenBlockchain BasicsAbhiNoch keine Bewertungen
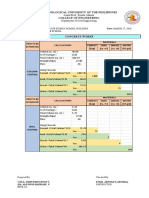
- 2 Concrete Works CompuDokument14 Seiten2 Concrete Works CompuALFONSO RAPHAEL SIANoch keine Bewertungen
- Core Java Vol 1 2 For The Impatient and Effective Pack 12Th Ed Cay S Horstmann Full ChapterDokument51 SeitenCore Java Vol 1 2 For The Impatient and Effective Pack 12Th Ed Cay S Horstmann Full Chapterkatherine.whipkey756100% (8)
- 310 - 010507 - 00001 - 01 - Technical Datasheet - Filterseparator SNP-PCH800.9Dokument8 Seiten310 - 010507 - 00001 - 01 - Technical Datasheet - Filterseparator SNP-PCH800.9Goulet KostNoch keine Bewertungen
- 11 Maintenance Strategy PDFDokument3 Seiten11 Maintenance Strategy PDFSaravanan RasayaNoch keine Bewertungen
- Contoh P&IDDokument1 SeiteContoh P&IDLudy Oji PrastamaNoch keine Bewertungen
- 4 Administration PDFDokument125 Seiten4 Administration PDFBojan BanjacNoch keine Bewertungen
- Mobile CommerceDokument47 SeitenMobile CommerceMichael DawkinsNoch keine Bewertungen
- HeroLab ManualDokument55 SeitenHeroLab ManualColin BraddockNoch keine Bewertungen
- CV-Agus Nugraha (11.01.2021)Dokument11 SeitenCV-Agus Nugraha (11.01.2021)Agus NugrahaNoch keine Bewertungen
- Agt Lim Katrin SaskiaDokument4 SeitenAgt Lim Katrin SaskiaJanine RoceroNoch keine Bewertungen
- SE Machine Advisor Node User ManualDokument90 SeitenSE Machine Advisor Node User ManualAlejandro RoalcabaNoch keine Bewertungen
- PUMP MMTV Vertical Mixed Flow Multistage Pump With CanisterDokument3 SeitenPUMP MMTV Vertical Mixed Flow Multistage Pump With Canisterarondaniel ocampoNoch keine Bewertungen
- IBM Tivoli Provisioning Manager V7.1.1 Deployment and IBM Service Management Integration Guide Sg247773Dokument762 SeitenIBM Tivoli Provisioning Manager V7.1.1 Deployment and IBM Service Management Integration Guide Sg247773bupbechanhNoch keine Bewertungen
- BTF PDFDokument4 SeitenBTF PDFArif PujiNoch keine Bewertungen
- Samsung Gb-19sen Chassis Le19r86bd LCDDokument117 SeitenSamsung Gb-19sen Chassis Le19r86bd LCDAntonio CersosimoNoch keine Bewertungen
- HiLook Product Catalog 2019H2 PDFDokument58 SeitenHiLook Product Catalog 2019H2 PDFCatur WijayaNoch keine Bewertungen
- LogDokument130 SeitenLogZaheerabbas KhanNoch keine Bewertungen
- AC 25.899-1 Electrical Bonding and Protection Against Static ElectricityDokument11 SeitenAC 25.899-1 Electrical Bonding and Protection Against Static ElectricitysheyunfengNoch keine Bewertungen
- Computer Education ModuleDokument22 SeitenComputer Education ModuleJulia Melissa CzapNoch keine Bewertungen
- RG Rap6262 (G) V1.1Dokument10 SeitenRG Rap6262 (G) V1.1July Esa PutraNoch keine Bewertungen