Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Malaria: Prima Dewi Yuliani 1210312120 Widyatul Aina Alfioni ParsiskaDokument27 SeitenMalaria: Prima Dewi Yuliani 1210312120 Widyatul Aina Alfioni ParsiskaAnonymous Di1zSIkRBHNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
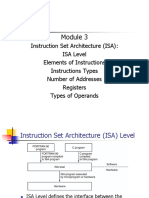
- Instruction Set Architecture (ISA) : ISA Level Elements of Instructions Instructions Types Number of Addresses Registers Types of OperandsDokument51 SeitenInstruction Set Architecture (ISA) : ISA Level Elements of Instructions Instructions Types Number of Addresses Registers Types of OperandsAnonymous Di1zSIkRBHNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Report of Treasurer RusDokument5 SeitenReport of Treasurer RusAnonymous Di1zSIkRBHNoch keine Bewertungen
- PLENO21CKULITDokument20 SeitenPLENO21CKULITAnonymous Di1zSIkRBHNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- After Studying This ChapterDokument2 SeitenAfter Studying This ChapterAnonymous Di1zSIkRBHNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Hepatoprotective Constituents of Firmiana Hepatocytes WebsiteDokument2 SeitenHepatoprotective Constituents of Firmiana Hepatocytes WebsiteAnonymous Di1zSIkRBHNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Slide Progosis Dan KomplikasDokument2 SeitenSlide Progosis Dan KomplikasAnonymous Di1zSIkRBHNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Inflation ExpectationsasaDokument29 SeitenInflation ExpectationsasaAnonymous Di1zSIkRBHNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- InfeksiDokument2 SeitenInfeksiAnonymous Di1zSIkRBHNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Quiz 5 Test BankDokument37 SeitenQuiz 5 Test BankOnyeka O AniyedeNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Anesthesia Management of Pregnant With HELLP Syndrome With Fetal Intrauterine Exitus (#1123666) - 2457074Dokument3 SeitenAnesthesia Management of Pregnant With HELLP Syndrome With Fetal Intrauterine Exitus (#1123666) - 2457074SALMA HANINANoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Document The FindingDokument25 SeitenDocument The Findingreenasree panneruNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- HELLP Syndrome Case Scenario 2AG1Dokument2 SeitenHELLP Syndrome Case Scenario 2AG1JR Rolf NeuqeletNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Hypertension in pregnancy-ACOG 2013-1 PDFDokument100 SeitenHypertension in pregnancy-ACOG 2013-1 PDFrabinreaganNoch keine Bewertungen
- Spontaneous Hepatic Rupture Associated With HELLP Syndrome: Britt C. Smyth, BA, RDMS, RVT, RDCSDokument3 SeitenSpontaneous Hepatic Rupture Associated With HELLP Syndrome: Britt C. Smyth, BA, RDMS, RVT, RDCSMetharisaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Nursing Care of A Family Experiencing A Sudden Pregnancy ComplicationDokument5 SeitenNursing Care of A Family Experiencing A Sudden Pregnancy ComplicationCrisheila Sarah PiedadNoch keine Bewertungen
- HELLP SyndromeDokument4 SeitenHELLP SyndromeDan Kenneth Liban LlantoNoch keine Bewertungen
- GestosisDokument15 SeitenGestosisjalan_zNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Plab-1 1700 MCQs Solved With Explanation (Shared by Ussama Maqbool)Dokument729 SeitenPlab-1 1700 MCQs Solved With Explanation (Shared by Ussama Maqbool)Omar Abo el nagaNoch keine Bewertungen
- High Risk Pregnancy Review QuestionsDokument59 SeitenHigh Risk Pregnancy Review Questionsmitted100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- SOMANZ - Hypertension Pregnancy Guideeline April 2014Dokument51 SeitenSOMANZ - Hypertension Pregnancy Guideeline April 2014Amanda Mustika AdiNoch keine Bewertungen
- Acog 19Dokument25 SeitenAcog 19Janet GoldameirNoch keine Bewertungen
- Edaic 3Dokument16 SeitenEdaic 3DsdNoch keine Bewertungen
- Pre EclampsiaDokument18 SeitenPre EclampsiaMary BlancoNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hypertensive Disorders in PregnancyDokument6 SeitenHypertensive Disorders in PregnancyLuiciaNoch keine Bewertungen
- Etiology and Management of Postpartum Hypertension-PreeclampsiaDokument6 SeitenEtiology and Management of Postpartum Hypertension-Preeclampsiawilliamjhon57Noch keine Bewertungen
- 1707 Question To Live in London-2 PDFDokument185 Seiten1707 Question To Live in London-2 PDFMorisse M MorisseNoch keine Bewertungen
- Gastrointestinal Diseases During Pregnancy What DoDokument11 SeitenGastrointestinal Diseases During Pregnancy What Dotakechi takechiNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- HematologyDokument58 SeitenHematologyAchmad DainuriNoch keine Bewertungen
- M1 Post Task - Caparas-Bsn2a-A2Dokument2 SeitenM1 Post Task - Caparas-Bsn2a-A2Gretta CaparasNoch keine Bewertungen
- Acute Fatty Liver of Pregnancy - V2.1 - GL780Dokument5 SeitenAcute Fatty Liver of Pregnancy - V2.1 - GL780Ade PurnaNoch keine Bewertungen
- 2 WA Pharmacological - and - Parenteral - Therapies - During - ChildbearingDokument27 Seiten2 WA Pharmacological - and - Parenteral - Therapies - During - ChildbearingLeigh ProsyneNoch keine Bewertungen
- Sush Unity Corrected OBS-GYN1700 PDFDokument218 SeitenSush Unity Corrected OBS-GYN1700 PDFUmer SaifullahNoch keine Bewertungen
- Hypertension in PregnancyDokument68 SeitenHypertension in PregnancyAbdul MoizNoch keine Bewertungen
- Hellp Syndrome and DicDokument5 SeitenHellp Syndrome and DicJanelle ArcillaNoch keine Bewertungen
- Acute Fatty Liver of Pregnancy A ThoroughDokument8 SeitenAcute Fatty Liver of Pregnancy A ThorougheeeeeeNoch keine Bewertungen
- Obstetric Anesthesia PDFDokument998 SeitenObstetric Anesthesia PDFFendy PrasetyoNoch keine Bewertungen
- Bare - The Blesser's Game - Jackie PhamotseDokument281 SeitenBare - The Blesser's Game - Jackie Phamotsetinyiko73% (126)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- HELLP!!!: A Case Study PresentationDokument32 SeitenHELLP!!!: A Case Study PresentationMaria Nena BalagtasNoch keine Bewertungen