Das könnte Ihnen auch gefallen
- Occupation in Occupational Therapy PDFDokument26 SeitenOccupation in Occupational Therapy PDFa_tobarNoch keine Bewertungen
- OT Models PratciceDokument30 SeitenOT Models PratciceWalaa Eldesoukey100% (1)
- Meaningful OccupationDokument13 SeitenMeaningful OccupationSyafiq Azzmi100% (1)
- The+Model+of+Creative+AbilityDokument22 SeitenThe+Model+of+Creative+AbilitysandeepNoch keine Bewertungen
- Model of Human OccupationDokument5 SeitenModel of Human OccupationPatrick IlaoNoch keine Bewertungen
- The Application of Assessment and Evaluation Procedure in Using Occupation Centered PracticeDokument55 SeitenThe Application of Assessment and Evaluation Procedure in Using Occupation Centered PracticeAswathi100% (1)
- Occupational Therapy ProcessDokument3 SeitenOccupational Therapy Processapi-339841373100% (1)
- The History of Occupational TherapyDokument17 SeitenThe History of Occupational TherapyHannah GuintoNoch keine Bewertungen
- A Case Study On Task Oriented ApproachDokument48 SeitenA Case Study On Task Oriented ApproachTIMOTHY NYONGESA0% (1)
- Occupation Based InterventionsDokument16 SeitenOccupation Based Interventionsapi-293182319100% (1)
- Task Oriented Approach PDFDokument21 SeitenTask Oriented Approach PDFAnditaNurfitri0% (1)
- Canadian Journal of Occupational TherapyDokument9 SeitenCanadian Journal of Occupational TherapyFrancesca GozmanNoch keine Bewertungen
- Canadian Occupational Performance Measure NOC LinkDokument3 SeitenCanadian Occupational Performance Measure NOC LinkRatna Sulistya DewiNoch keine Bewertungen
- Study ResourcesDokument3 SeitenStudy Resourcesapi-405162391Noch keine Bewertungen
- Mosey's Developmental GroupsDokument3 SeitenMosey's Developmental Groupsedwin.roc523100% (2)
- Assessing Functional AbilityDokument15 SeitenAssessing Functional AbilitySonali Soumyashree100% (2)
- Uniform Terminology AOTA PDFDokument8 SeitenUniform Terminology AOTA PDFLaura GuevaraNoch keine Bewertungen
- Developmental Approach or Frame of ReferenceDokument27 SeitenDevelopmental Approach or Frame of ReferenceHEMA CHANDRANNoch keine Bewertungen
- Occupations Across The LifespanDokument6 SeitenOccupations Across The LifespanMary Elizabeth JoyceNoch keine Bewertungen
- Frame of ReferenceDokument10 SeitenFrame of ReferenceGustavo CabanasNoch keine Bewertungen
- CMOP-E occupational model overviewDokument16 SeitenCMOP-E occupational model overviewAnca-Maria Vlad100% (2)
- 2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)Dokument54 Seiten2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)engshi18Noch keine Bewertungen
- History of OT Infographic TimelineDokument1 SeiteHistory of OT Infographic TimelineAddissa MarieNoch keine Bewertungen
- Ota Group ProtocolDokument26 SeitenOta Group Protocolapi-318685839Noch keine Bewertungen
- Working As An Occupational Therapist in Another Country 2015Dokument101 SeitenWorking As An Occupational Therapist in Another Country 2015RLedgerdNoch keine Bewertungen
- Community Mental HealthDokument2 SeitenCommunity Mental HealthGhea Mae Jukebox VillasNoch keine Bewertungen
- Implementing Occupation-Based PracticeDokument10 SeitenImplementing Occupation-Based Practiceapi-392268685Noch keine Bewertungen
- The Canadian Model of Occupational Performance and EngagementDokument16 SeitenThe Canadian Model of Occupational Performance and Engagementalepati29Noch keine Bewertungen
- 2012 Practice Analysis Executive Otr PDFDokument32 Seiten2012 Practice Analysis Executive Otr PDFRuxandra PredaNoch keine Bewertungen
- AOTA Statement On Role of OT in NICUDokument9 SeitenAOTA Statement On Role of OT in NICUMapi RuizNoch keine Bewertungen
- Motor Control ApproachesDokument26 SeitenMotor Control ApproachesAlyssa ArroyoNoch keine Bewertungen
- Occupational Therapy and Mental Health - Add Summary and Bullet PointsDokument11 SeitenOccupational Therapy and Mental Health - Add Summary and Bullet Pointsapi-339190475100% (1)
- Prevalence of Dyslexia Among Primary School ChildrenDokument19 SeitenPrevalence of Dyslexia Among Primary School ChildrenJubie MathewNoch keine Bewertungen
- Occupational Therapy in Pain ManagementDokument26 SeitenOccupational Therapy in Pain ManagementNoor Emellia JamaludinNoch keine Bewertungen
- Presented By: Ashlee Barbeau Student Occupational Therapist, Queen's UniversityDokument22 SeitenPresented By: Ashlee Barbeau Student Occupational Therapist, Queen's UniversityDanielle Stella N'LucaNoch keine Bewertungen
- Motor Learning Theory: References: Cole & Tufano, Chapter 19 Reserve Article: Mathiowetz & Bass Haugen (1994) AJOTDokument27 SeitenMotor Learning Theory: References: Cole & Tufano, Chapter 19 Reserve Article: Mathiowetz & Bass Haugen (1994) AJOTSundar SweeNoch keine Bewertungen
- School BasedOccupationalTherapyduringCOVID 19Dokument12 SeitenSchool BasedOccupationalTherapyduringCOVID 19Ligia SendreaNoch keine Bewertungen
- Soap 11Dokument4 SeitenSoap 11api-436429414Noch keine Bewertungen
- 2019 - Csusm Gmail Email Resume I Placed On Weebly With Better ObjectiveDokument2 Seiten2019 - Csusm Gmail Email Resume I Placed On Weebly With Better Objectiveapi-406769716Noch keine Bewertungen
- Aota PDFDokument2 SeitenAota PDFJuliana MassariolliNoch keine Bewertungen
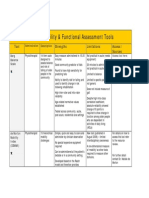
- Assessment Tools for Mobility & Functional IndependenceDokument4 SeitenAssessment Tools for Mobility & Functional Independencesonya63265Noch keine Bewertungen
- OT Frames Rehab BiomechanicalDokument18 SeitenOT Frames Rehab BiomechanicalCaryssa Vitelli100% (1)
- Occupational AdaptationDokument5 SeitenOccupational AdaptationVASH12345100% (1)
- Article 1Dokument7 SeitenArticle 1dguginNoch keine Bewertungen
- Effectiveness of Occupation-Based Interventions To Improve Areas of Occupation and Social Participation After StrokeDokument11 SeitenEffectiveness of Occupation-Based Interventions To Improve Areas of Occupation and Social Participation After StrokeSandra BarbazanNoch keine Bewertungen
- Chapter 16: Application of Motor Control and Motor LearningDokument8 SeitenChapter 16: Application of Motor Control and Motor LearningJireh Chambers100% (1)
- Occupational Therapy Association of The PhilippinesDokument12 SeitenOccupational Therapy Association of The PhilippinesChia ChangNoch keine Bewertungen
- Occupational Therapy As A Major Activity of Human Being: by Rafia KhalidDokument20 SeitenOccupational Therapy As A Major Activity of Human Being: by Rafia Khalidnomi9818Noch keine Bewertungen
- Group 3's Presentation on the Model of Human OccupationDokument21 SeitenGroup 3's Presentation on the Model of Human OccupationDEVORAH CARUZNoch keine Bewertungen
- The Biomechanical ModelDokument17 SeitenThe Biomechanical ModelLama NammouraNoch keine Bewertungen
- Pub - Qualitative Research in Evidence Based Rehabilitat PDFDokument156 SeitenPub - Qualitative Research in Evidence Based Rehabilitat PDFgstam69100% (1)
- Canadian Occupational Performance Measure (COPM) : 4 EditionDokument3 SeitenCanadian Occupational Performance Measure (COPM) : 4 EditionDulcea LoredanaNoch keine Bewertungen
- Soap Note 2 Community ClientDokument12 SeitenSoap Note 2 Community Clientapi-271984934Noch keine Bewertungen
- Occupational Therapy in Child Psychiatry (Emellia)Dokument19 SeitenOccupational Therapy in Child Psychiatry (Emellia)Noor Emellia JamaludinNoch keine Bewertungen
- Fisher (2013) Occupation-Centred Occupation-Based Occupation-FocusedDokument12 SeitenFisher (2013) Occupation-Centred Occupation-Based Occupation-FocusedElianaMicaela100% (1)
- Australian occupational therapy competency standards 2018Dokument16 SeitenAustralian occupational therapy competency standards 2018Mochammad Syarif HidayatNoch keine Bewertungen
- PTH 870-Occupational TherapyDokument13 SeitenPTH 870-Occupational Therapyapi-551496110100% (1)
- Cognitive Rehabilitation For Occupational Outcomes After Traumatic Brain InjuryDokument9 SeitenCognitive Rehabilitation For Occupational Outcomes After Traumatic Brain InjuryHardeep Singh BaliNoch keine Bewertungen
- Barthel vs. FIMDokument5 SeitenBarthel vs. FIMFrancisco CampoverdeNoch keine Bewertungen
- Rheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementVon EverandRheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementLynne GoodacreNoch keine Bewertungen
- CV - Vicky Chu - 朱薇錡Dokument2 SeitenCV - Vicky Chu - 朱薇錡Caesar HsiaoNoch keine Bewertungen
- Seminars Trainings Classroom Discussion: Training and Development ProgramsDokument2 SeitenSeminars Trainings Classroom Discussion: Training and Development ProgramsClarice LangitNoch keine Bewertungen
- Lomba Pidato Bhs InggrisDokument8 SeitenLomba Pidato Bhs Inggrissdn neg01Noch keine Bewertungen
- Indicators of Effectiveness:: A Practical Worksheet For Foundation Staff and BoardDokument4 SeitenIndicators of Effectiveness:: A Practical Worksheet For Foundation Staff and BoardTeachers Without BordersNoch keine Bewertungen
- 40 Great Education Research Paper TopicsDokument25 Seiten40 Great Education Research Paper TopicsMagelyn NBNoch keine Bewertungen
- LEARNING PLAN IN TLE 10 4th QDokument4 SeitenLEARNING PLAN IN TLE 10 4th QMa'am MabelNoch keine Bewertungen
- L. Jonathan Cohen - The Probable and The Provable-Oxford University Press, USA (1977)Dokument392 SeitenL. Jonathan Cohen - The Probable and The Provable-Oxford University Press, USA (1977)Giovanni Americo Bautista Pari100% (1)
- Personality DevelopmentDokument6 SeitenPersonality DevelopmentAnusha Verghese100% (1)
- Contemporary Comparative Education-Ppt CezDokument7 SeitenContemporary Comparative Education-Ppt CezCECILIA FE BERNAL100% (1)
- Scei ModelDokument9 SeitenScei ModelCalistus Eugene FernandoNoch keine Bewertungen
- Andrea Villarreal Resume 2014Dokument2 SeitenAndrea Villarreal Resume 2014api-257114951Noch keine Bewertungen
- Experimental Project On Action ResearchDokument3 SeitenExperimental Project On Action Researchddum292Noch keine Bewertungen
- Leila Ponsford 2016-2017Dokument3 SeitenLeila Ponsford 2016-2017api-267808262Noch keine Bewertungen
- Sample Paper Syllabus 2020-21: ClassDokument2 SeitenSample Paper Syllabus 2020-21: ClassBalachandranNoch keine Bewertungen
- Kubler-Ross-Change-Curve - Emotional Change PDFDokument1 SeiteKubler-Ross-Change-Curve - Emotional Change PDFbresmanNoch keine Bewertungen
- Enhancing Student Learning Experience and Satisfaction Using Virtual Learning EnvironmentsDokument2 SeitenEnhancing Student Learning Experience and Satisfaction Using Virtual Learning Environments- -Noch keine Bewertungen
- Reflection On My Experience of Oral PresentationDokument4 SeitenReflection On My Experience of Oral PresentationAssignmentLab.comNoch keine Bewertungen
- Development of Early Childhood Educaton: No. Matrikulasi: No. Kad Pengnealan: No. Telefon: E-MelDokument7 SeitenDevelopment of Early Childhood Educaton: No. Matrikulasi: No. Kad Pengnealan: No. Telefon: E-Mel黄珮珊Noch keine Bewertungen
- Effect of Visual Attributes On Zero Shot Learning Jacob ChandranDokument20 SeitenEffect of Visual Attributes On Zero Shot Learning Jacob Chandranapi-282127378Noch keine Bewertungen
- Ahmed Ismail: Chinese-Arabic Interpretation TranslatorDokument2 SeitenAhmed Ismail: Chinese-Arabic Interpretation TranslatorAbdulrahman TahaNoch keine Bewertungen
- Hebb Neural Network: Learning and ApplicationsDokument12 SeitenHebb Neural Network: Learning and ApplicationsVighnesh MNoch keine Bewertungen
- Motivational Letter - L.GDokument2 SeitenMotivational Letter - L.GFilip DinevNoch keine Bewertungen
- Neurobiology of Emotional Trauma ReviewDokument10 SeitenNeurobiology of Emotional Trauma Reviewfreudpoe37Noch keine Bewertungen
- Teachers EfficacyDokument29 SeitenTeachers EfficacyBhannu RamananNoch keine Bewertungen
- Prelim Exam TauracDokument4 SeitenPrelim Exam TauracNorjanah TauracNoch keine Bewertungen
- Your First Day at WorkDokument10 SeitenYour First Day at WorkPhu Cong LeNoch keine Bewertungen
- Mind FullnessDokument4 SeitenMind FullnessApp SoulsNoch keine Bewertungen
- Fostering An Innovative OrganisationDokument29 SeitenFostering An Innovative OrganisationM Aamir AsgharNoch keine Bewertungen
- English4 - Q1 CoT Plan 1 2022Dokument3 SeitenEnglish4 - Q1 CoT Plan 1 2022juliet diaz100% (1)
- Seating Arrangement and Question-Asking: Learning Environments Research 2: 249-263, 2000Dokument16 SeitenSeating Arrangement and Question-Asking: Learning Environments Research 2: 249-263, 2000RyskaAlNurfiantyNoch keine Bewertungen