Das könnte Ihnen auch gefallen
- American Ent Oxford PDFDokument461 SeitenAmerican Ent Oxford PDFanna100% (3)
- Brain Bee NotesDokument10 SeitenBrain Bee Notesapi-534972164Noch keine Bewertungen
- Neurology Short NotesDokument11 SeitenNeurology Short NotesSachin Kumar Rastogi100% (1)
- CARAS SCUTSHEET 2nd EditDokument2 SeitenCARAS SCUTSHEET 2nd EditFrances Katrina Siruno100% (1)
- Past MCQs On Ocular AnatomyDokument7 SeitenPast MCQs On Ocular AnatomyEliza Spark33% (6)
- Cranial NervesDokument14 SeitenCranial NervesIrina Garlea-Robu100% (1)
- Cranial Nerve ExaminationDokument3 SeitenCranial Nerve Examinationapi-195986134Noch keine Bewertungen
- Cranial Nerve Exam in DetailDokument36 SeitenCranial Nerve Exam in DetailANIE100% (1)
- Complete Neurologic ExamDokument21 SeitenComplete Neurologic ExamRaymond CruzNoch keine Bewertungen
- Neurological ExaminationDokument240 SeitenNeurological Examinationramadan0% (1)
- Cranial Nerves ListDokument4 SeitenCranial Nerves Listashdmb217Noch keine Bewertungen
- MS Myasthenia Gravis Gillian-Barre Syndrome Parkinson's: Ascending Reversible ParalysisDokument5 SeitenMS Myasthenia Gravis Gillian-Barre Syndrome Parkinson's: Ascending Reversible ParalysishaxxxessNoch keine Bewertungen
- Neurology Shelf Exam Review - Part 2.newDokument14 SeitenNeurology Shelf Exam Review - Part 2.newyogurtNoch keine Bewertungen
- Headache: Differential Diagnosis of HeadacheDokument139 SeitenHeadache: Differential Diagnosis of Headachemero1983Noch keine Bewertungen
- Cranial Nerves: General CharacteristicsDokument17 SeitenCranial Nerves: General CharacteristicsRiki AntoNoch keine Bewertungen
- Neurological Examination: ObserveDokument9 SeitenNeurological Examination: ObserveTom MallinsonNoch keine Bewertungen
- Diagnostic Approach To HeadacheDokument7 SeitenDiagnostic Approach To HeadachedanlaytonNoch keine Bewertungen
- Head To Toe AssessmentDokument22 SeitenHead To Toe AssessmentNessa Layos MorilloNoch keine Bewertungen
- OSCE Cerebellar Examination PDFDokument6 SeitenOSCE Cerebellar Examination PDFriczen vilaNoch keine Bewertungen
- Neurological Physical ExamDokument3 SeitenNeurological Physical Examjyhn24Noch keine Bewertungen
- Neurology - Saif.wesmosis.2013 104907Dokument68 SeitenNeurology - Saif.wesmosis.2013 104907Helene AlawamiNoch keine Bewertungen
- Neuro Assess HandoutDokument14 SeitenNeuro Assess HandoutPie ArtWorkNoch keine Bewertungen
- Health HistoryDokument19 SeitenHealth HistoryAngelene Caliva100% (1)
- Cranial Nerve Examination Part IDokument91 SeitenCranial Nerve Examination Part IAARYA100% (1)
- 140 - Neurology Pathology) Seizures - Etiology, Pathophysiology, Clinical Features, Treatment, ComplicationsDokument10 Seiten140 - Neurology Pathology) Seizures - Etiology, Pathophysiology, Clinical Features, Treatment, ComplicationsUssama MDNoch keine Bewertungen
- Rosh NeuroDokument11 SeitenRosh NeuroSoni AliNoch keine Bewertungen
- Lesion Localization in NeurologyDokument34 SeitenLesion Localization in NeurologyValeria Leon AbadNoch keine Bewertungen
- (MicroB) Brainstem Lesions - Dr. Bravo (Nico Castillo)Dokument4 Seiten(MicroB) Brainstem Lesions - Dr. Bravo (Nico Castillo)miguel cuevasNoch keine Bewertungen
- Summary of Cranial NervesDokument1 SeiteSummary of Cranial NervesjackieNoch keine Bewertungen
- Headache: Rosen's Chapters 17 and 105 November 9, 2006 by George FiliadisDokument45 SeitenHeadache: Rosen's Chapters 17 and 105 November 9, 2006 by George Filiadishemanthshah2801Noch keine Bewertungen
- Anatomy of Cerebral Blood Supply & Cerebral PhysiologyDokument32 SeitenAnatomy of Cerebral Blood Supply & Cerebral Physiologykiran kizhakkiniNoch keine Bewertungen
- Nerve Components Location of Nerve Cell Bodies Cranial Exit Main Action(s)Dokument3 SeitenNerve Components Location of Nerve Cell Bodies Cranial Exit Main Action(s)Tan En YingNoch keine Bewertungen
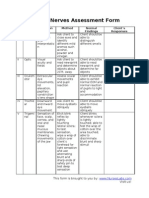
- Cranial Nerves Assessment FormDokument3 SeitenCranial Nerves Assessment Formmhel03_chickmagnetNoch keine Bewertungen
- Step-Wise Approaches in Clinical Examination - SampleDokument8 SeitenStep-Wise Approaches in Clinical Examination - Samplecsbully913Noch keine Bewertungen
- Mnemonic For Medical Students For Upper and Lower Motor LesionsDokument1 SeiteMnemonic For Medical Students For Upper and Lower Motor LesionsLe-Ann Mariamlelue100% (2)
- (MicroB) 3.6 Brainstem LesionsDokument6 Seiten(MicroB) 3.6 Brainstem Lesionsnelson lopezNoch keine Bewertungen
- The Brain and Cranial NervesDokument4 SeitenThe Brain and Cranial NervesJet ToralbaNoch keine Bewertungen
- Neuro 101: Nursing Neuro Assessment: Kristen Ankrom, RN, SCRN, CCCC Stroke Coordinator Coliseum Medical CentersDokument29 SeitenNeuro 101: Nursing Neuro Assessment: Kristen Ankrom, RN, SCRN, CCCC Stroke Coordinator Coliseum Medical CentersDarvin MathewNoch keine Bewertungen
- Neurology Cram NotesDokument19 SeitenNeurology Cram Notesrjh1895Noch keine Bewertungen
- Examination of The Peripheral Neurological SystemDokument2 SeitenExamination of The Peripheral Neurological Systemkenners100% (12)
- Localisation in NeurologyDokument19 SeitenLocalisation in NeurologyArnav GuptaNoch keine Bewertungen
- Kathynotes PDFDokument103 SeitenKathynotes PDFvarrakeshNoch keine Bewertungen
- Clinical Neurology Answers OnlyDokument68 SeitenClinical Neurology Answers Onlyanas kNoch keine Bewertungen
- Increased ICP: A) HeadacheDokument5 SeitenIncreased ICP: A) Headachemohamed nagyNoch keine Bewertungen
- PNS Examination 15Dokument17 SeitenPNS Examination 15NolanNoch keine Bewertungen
- Dementia Evaluation and TreatmentDokument12 SeitenDementia Evaluation and Treatmentrofi modiNoch keine Bewertungen
- Antiepileptics (Autosaved)Dokument57 SeitenAntiepileptics (Autosaved)vishal singhNoch keine Bewertungen
- Cranial Nerves: DR - Ahmed Gaber Ass. Prof of Neurology Ain Shams UniversityDokument45 SeitenCranial Nerves: DR - Ahmed Gaber Ass. Prof of Neurology Ain Shams UniversityKhaled OssamaNoch keine Bewertungen
- Cranial Nerve ExaminationDokument19 SeitenCranial Nerve ExaminationBhargavi SoodNoch keine Bewertungen
- Autonomic and Systemic Pharmacology DR DahalDokument119 SeitenAutonomic and Systemic Pharmacology DR Dahalअविनाश भाल्टरNoch keine Bewertungen
- Essential Tremor Diagnosis and TreatmentDokument32 SeitenEssential Tremor Diagnosis and TreatmentAntony JebarajNoch keine Bewertungen
- Glutamate: Neurotransmitters Disturbed Increased Sympathetic Stimulation Increased Autonomic StimulationDokument3 SeitenGlutamate: Neurotransmitters Disturbed Increased Sympathetic Stimulation Increased Autonomic StimulationCM NajitoNoch keine Bewertungen
- Neurology in TableDokument93 SeitenNeurology in TableHassan Bani SaeidNoch keine Bewertungen
- Medicine1 Grand PE ScriptDokument10 SeitenMedicine1 Grand PE ScriptCarmeline Santi BeronillaNoch keine Bewertungen
- Source NotesDokument30 SeitenSource NotesChris Jardine Li100% (1)
- VertigoDokument50 SeitenVertigosaltoftheearthlightoftheworld506Noch keine Bewertungen
- Antiseizure, Sedative & HypnoticsDokument8 SeitenAntiseizure, Sedative & HypnoticsThulasi tootsieNoch keine Bewertungen
- Neuro DDXDokument5 SeitenNeuro DDXDDXNoch keine Bewertungen
- Ring Enhancing LesionsDokument50 SeitenRing Enhancing LesionsVivek GuptaNoch keine Bewertungen
- Spinal Cord: Anatomy and NeuroimagingDokument52 SeitenSpinal Cord: Anatomy and NeuroimagingslojnotakNoch keine Bewertungen
- PRES (Posterior Reversible Encephalopathy Syndrome) and Eclampsia-ReviewDokument5 SeitenPRES (Posterior Reversible Encephalopathy Syndrome) and Eclampsia-ReviewAvicena M IqbalNoch keine Bewertungen
- Micro para Questions 2004 2005Dokument6 SeitenMicro para Questions 2004 2005DonnaBells Hermo LabaniegoNoch keine Bewertungen
- Medical Micro-Apmc QuestionsDokument8 SeitenMedical Micro-Apmc QuestionsDonnaBells Hermo LabaniegoNoch keine Bewertungen
- Physician's Licensure Exam. For Micro-ParaDokument4 SeitenPhysician's Licensure Exam. For Micro-ParaDonnaBells Hermo LabaniegoNoch keine Bewertungen
- StrokeDokument74 SeitenStrokeDonnaBells Hermo Labaniego100% (2)
- B11Ph02 AntihelmenticsDokument6 SeitenB11Ph02 AntihelmenticsDonnaBells Hermo LabaniegoNoch keine Bewertungen
- Praise and Worship SongsDokument7 SeitenPraise and Worship SongsDonnaBells Hermo LabaniegoNoch keine Bewertungen
- Family PlanningDokument98 SeitenFamily PlanningDonnaBells Hermo Labaniego50% (2)
- Biological Psychology Lesson 5 NotesDokument24 SeitenBiological Psychology Lesson 5 Notesjeyn100% (1)
- Nervous System Detailed Lesson Plan OrigDokument13 SeitenNervous System Detailed Lesson Plan OrigEdnalyn Licot100% (1)
- CH 14: Spinal Cord and Spinal NervesDokument15 SeitenCH 14: Spinal Cord and Spinal NervesNoman khanNoch keine Bewertungen
- Head and Neck Cancer - Reconstruction: HistoryDokument6 SeitenHead and Neck Cancer - Reconstruction: HistorySri MahyantiNoch keine Bewertungen
- Prepared By:: - Mohammad Waqas Lari - Karachi Med & DentalDokument18 SeitenPrepared By:: - Mohammad Waqas Lari - Karachi Med & DentalalirazanaqwiNoch keine Bewertungen
- (Inc. Barcharts) Senses Laminated Reference Guide (Z Lib - Org)Dokument2 Seiten(Inc. Barcharts) Senses Laminated Reference Guide (Z Lib - Org)Camilo Ignacio Arriagada Jara100% (1)
- Examination of Salivary GlandsDokument29 SeitenExamination of Salivary GlandsSamchristy MammenNoch keine Bewertungen
- PNS RSO LectureDokument40 SeitenPNS RSO LectureIvan de GranoNoch keine Bewertungen
- AOI APState August10Dokument141 SeitenAOI APState August10Anoop BabuNoch keine Bewertungen
- AnaphyDokument8 SeitenAnaphyCELLINA CLARISSE DE LEONNoch keine Bewertungen
- The Respiratory System of OxDokument14 SeitenThe Respiratory System of OxHemant JoshiNoch keine Bewertungen
- Lecture 5 The Respiratory SystemDokument4 SeitenLecture 5 The Respiratory Systemmido_20067581Noch keine Bewertungen
- Thru S-S Pivot - Jugular ProcessesDokument5 SeitenThru S-S Pivot - Jugular ProcessesveronicaNoch keine Bewertungen
- Tracheostomy Care: PhysiologyDokument2 SeitenTracheostomy Care: PhysiologyrajirajeshNoch keine Bewertungen
- Thyroid CrisisDokument17 SeitenThyroid CrisisFebriliana Mao-maoNoch keine Bewertungen
- Ear Trauma: Kylee Eagles,, Laura Fralich,, J. Herbert StevensonDokument14 SeitenEar Trauma: Kylee Eagles,, Laura Fralich,, J. Herbert StevensonInggitaDarmawanNoch keine Bewertungen
- Olfactory Outcomes After Middle Turbinate Resection in Endoscopic Transsphenoidal Surgery: A Prospective Randomized StudyDokument7 SeitenOlfactory Outcomes After Middle Turbinate Resection in Endoscopic Transsphenoidal Surgery: A Prospective Randomized Studypaul00040Noch keine Bewertungen
- Dr. Rahmi Ardhini, SPSDokument60 SeitenDr. Rahmi Ardhini, SPSsatyagraha84Noch keine Bewertungen
- Cholesteatoma Part 5 Congenital Cholesteatoma PDFDokument4 SeitenCholesteatoma Part 5 Congenital Cholesteatoma PDFSuprit Sn100% (1)
- Aphasia 07Dokument34 SeitenAphasia 07razik89Noch keine Bewertungen
- Hypergraphia: Contributors To Wikimedia ProjectsDokument8 SeitenHypergraphia: Contributors To Wikimedia ProjectsCool ArticNoch keine Bewertungen
- Neurophysiology: Motor Neurophysiology: BIOE 3340Dokument60 SeitenNeurophysiology: Motor Neurophysiology: BIOE 3340sam manNoch keine Bewertungen
- Tumours of HypopharynxDokument32 SeitenTumours of HypopharynxDurrikamil khattakNoch keine Bewertungen
- Neck DissectionDokument51 SeitenNeck DissectionRakshith12Noch keine Bewertungen
- CerebellumDokument22 SeitenCerebellumJasvinder Singh NayyarNoch keine Bewertungen
- 2022-Pricelist Feb2022 PDFDokument2 Seiten2022-Pricelist Feb2022 PDFjackNoch keine Bewertungen
- Session 2 TMJDokument5 SeitenSession 2 TMJTobio KageyamaNoch keine Bewertungen