Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hoferl 2015Dokument6 SeitenHoferl 2015SitiKhadijahNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- DfsdfsDokument12 SeitenDfsdfsSitiKhadijahNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Restoring Worn Dentition: Assessing Occlusion's RoleDokument125 SeitenRestoring Worn Dentition: Assessing Occlusion's RoleSitiKhadijahNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Review Article: A New Classification of Endodontic-Periodontal LesionsDokument6 SeitenReview Article: A New Classification of Endodontic-Periodontal LesionsSitiKhadijahNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- X-Smart Plus Brochure Maillefer Badge enDokument3 SeitenX-Smart Plus Brochure Maillefer Badge enSitiKhadijahNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- 90Dokument5 Seiten90SitiKhadijahNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- 2004 EndodtopicsHaapasaloetalDokument8 Seiten2004 EndodtopicsHaapasaloetalSitiKhadijahNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Boss Hard 2017Dokument10 SeitenBoss Hard 2017SitiKhadijahNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Christensen 2008Dokument4 SeitenChristensen 2008SitiKhadijahNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- 2004 EndodtopicsHaapasaloetal PDFDokument28 Seiten2004 EndodtopicsHaapasaloetal PDFSitiKhadijahNoch keine Bewertungen
- Sol Ruz 2015Dokument7 SeitenSol Ruz 2015SitiKhadijahNoch keine Bewertungen
- Fracture Reaons in PFMDokument5 SeitenFracture Reaons in PFMShounak GhoshNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Implant-Retained Cantilever Fixed Prosthesis: Where and WhenDokument4 SeitenImplant-Retained Cantilever Fixed Prosthesis: Where and WhenSitiKhadijahNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Identification of Complete Denture Problems: A Summary: ProstheticsDokument7 SeitenIdentification of Complete Denture Problems: A Summary: ProstheticsPolo RalfNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- CantileverDokument6 SeitenCantileverSitiKhadijahNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Gurrea Bruguera IJED 2014Dokument18 SeitenGurrea Bruguera IJED 2014SitiKhadijahNoch keine Bewertungen
- f26f PDFDokument9 Seitenf26f PDFSitiKhadijahNoch keine Bewertungen
- 1548 FullDokument9 Seiten1548 FullSitiKhadijahNoch keine Bewertungen
- 2014 02 05 LimTongWahDokument6 Seiten2014 02 05 LimTongWahSitiKhadijahNoch keine Bewertungen
- BDA Occlusion Seminar 2Dokument88 SeitenBDA Occlusion Seminar 2SitiKhadijahNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Effect of EDTA Sodium Hypochlorite and C PDFDokument4 SeitenEffect of EDTA Sodium Hypochlorite and C PDFZulfahmi NurdinNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Managment of Wear2Dokument7 SeitenManagment of Wear2hmsatNoch keine Bewertungen
- Applied-A Comparative Evaluation-Shweta BagmarDokument8 SeitenApplied-A Comparative Evaluation-Shweta BagmarImpact JournalsNoch keine Bewertungen
- Removable Prostheses: Tooth Surface LossDokument4 SeitenRemovable Prostheses: Tooth Surface LossSitiKhadijahNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- 10 1046@j 1365-2591 2000 00273 XDokument7 Seiten10 1046@j 1365-2591 2000 00273 XSitiKhadijahNoch keine Bewertungen
- Christensen 2009Dokument4 SeitenChristensen 2009SitiKhadijahNoch keine Bewertungen
- TJ Der Hane 2009Dokument33 SeitenTJ Der Hane 2009SitiKhadijahNoch keine Bewertungen
- Ataali 2014Dokument9 SeitenAtaali 2014SitiKhadijahNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Mixed Designs: Between and Within: Psy 420 AinsworthDokument30 SeitenMixed Designs: Between and Within: Psy 420 AinsworthSitiKhadijahNoch keine Bewertungen
- 11 SPSS Procedure For Kruskal Wallis TestDokument5 Seiten11 SPSS Procedure For Kruskal Wallis TestSitiKhadijahNoch keine Bewertungen
- Nursing Care PlanDokument14 SeitenNursing Care PlanMaria Pina Barbado PonceNoch keine Bewertungen
- Kitchen Safety: Precautions and First Aid: Study Guide L Module No.5Dokument12 SeitenKitchen Safety: Precautions and First Aid: Study Guide L Module No.5Marlyn MabalotNoch keine Bewertungen
- Flashcard ATLS Pretest - QuizletDokument14 SeitenFlashcard ATLS Pretest - QuizletAnonymous QCi88VHNoch keine Bewertungen
- Rules For Scoring Respiratory Events in Sleep: Update of The 2007 AASM Manual For The Scoring of Sleep and Associated EventsDokument23 SeitenRules For Scoring Respiratory Events in Sleep: Update of The 2007 AASM Manual For The Scoring of Sleep and Associated Eventsgiulio pinnolaNoch keine Bewertungen
- 1 Medical-PräsentDokument84 Seiten1 Medical-PräsentpurplefokNoch keine Bewertungen
- Diseases of Respiratory SystemDokument34 SeitenDiseases of Respiratory SystemJerrald Meyer L. BayaniNoch keine Bewertungen
- PDFsam MergeDokument47 SeitenPDFsam MergeAyman JadNoch keine Bewertungen
- Autacoids & RSDokument14 SeitenAutacoids & RSIsmail Bazly ZarirNoch keine Bewertungen
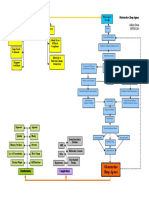
- Sleep Apnea Concept MapDokument1 SeiteSleep Apnea Concept Mapashleydean100% (2)
- Diver Medic BrochureDokument7 SeitenDiver Medic BrochureFernando Cadena DuqueNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 6-Minute Walk Test in Patients With COPD: Clinical Applications in Pulmonary RehabilitationDokument8 Seiten6-Minute Walk Test in Patients With COPD: Clinical Applications in Pulmonary RehabilitationFriendlymeNoch keine Bewertungen
- JHA For Tiling WorkDokument1 SeiteJHA For Tiling WorkMuhammad Suffyanazwan80% (5)
- Sunflag Chemicals Pvt. LTDDokument5 SeitenSunflag Chemicals Pvt. LTDkunalNoch keine Bewertungen
- Assessment Subjective: "Nahihirapan Ako Huminga" As VerbalizedDokument2 SeitenAssessment Subjective: "Nahihirapan Ako Huminga" As Verbalizedmayla_jordan3666Noch keine Bewertungen
- Adult BLSDokument32 SeitenAdult BLSMel GaholNoch keine Bewertungen
- First AidDokument2 SeitenFirst AidHannah DuyagNoch keine Bewertungen
- Inhaled Corticosteroids and Voice Problems. What Is New - PDFDokument7 SeitenInhaled Corticosteroids and Voice Problems. What Is New - PDFDaniel Celestino DiazNoch keine Bewertungen
- Role Play Bahasa Inggris " Staf Rumah Sakit ": Disusun OlehDokument6 SeitenRole Play Bahasa Inggris " Staf Rumah Sakit ": Disusun OlehRokhma mistaNoch keine Bewertungen
- Pyridine PDFDokument6 SeitenPyridine PDFanon_342721354Noch keine Bewertungen
- Clinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test BankDokument9 SeitenClinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test Banksarahpalmerotpdkjcwfq100% (24)
- Quizlet 20 PDFDokument9 SeitenQuizlet 20 PDFSarath kumarNoch keine Bewertungen
- Santovac 5 SDS PDFDokument5 SeitenSantovac 5 SDS PDFmanish_keswani01Noch keine Bewertungen
- Safety Data Sheet for Sasfroth 39Dokument16 SeitenSafety Data Sheet for Sasfroth 39Mark KuttinNoch keine Bewertungen
- Identification of The Material and Supplier: SDS Date: 14 Jan 2017 Version No: 3 of 6Dokument6 SeitenIdentification of The Material and Supplier: SDS Date: 14 Jan 2017 Version No: 3 of 6LABORATORIUM FERTILINDONoch keine Bewertungen
- M 06536 A CT Lung Imaging Temporary 90 Day License PDFDokument2 SeitenM 06536 A CT Lung Imaging Temporary 90 Day License PDFMerim JusufbegovicNoch keine Bewertungen
- MSDS Sikaflex-211-SWDokument11 SeitenMSDS Sikaflex-211-SWandreankerjaNoch keine Bewertungen
- Living Like The Tortoise Doubling Your Life SpanDokument5 SeitenLiving Like The Tortoise Doubling Your Life SpanJihane Z100% (1)
- QuestionsDokument4 SeitenQuestionsKeerthi Chowdary AmaraneniNoch keine Bewertungen
- Ultrasonic Cleaning Solution, MC-3 - Metal Cleaner - SdsDokument5 SeitenUltrasonic Cleaning Solution, MC-3 - Metal Cleaner - SdsLaban KantorNoch keine Bewertungen
- High Altitude Environment Physiology, Adaptations, and IllnessDokument3 SeitenHigh Altitude Environment Physiology, Adaptations, and IllnessJoseph AmeerNoch keine Bewertungen
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (13)