Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- I10 Workshop Manual - ADokument292 SeitenI10 Workshop Manual - ANorthstartechnology Company82% (11)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Lacosamide 1Dokument6 SeitenLacosamide 1ezio93Noch keine Bewertungen
- Neuropsychologia: Cheryl L. Grady, Catherine J. Mondloch, Terri L. Lewis, Daphne MaurerDokument18 SeitenNeuropsychologia: Cheryl L. Grady, Catherine J. Mondloch, Terri L. Lewis, Daphne MaurerPutri AdnyaniNoch keine Bewertungen
- Domes 2013 Emotional Empathy and Psychopathy in OffendersDokument18 SeitenDomes 2013 Emotional Empathy and Psychopathy in OffendersPutri AdnyaniNoch keine Bewertungen
- Jurnal 2Dokument10 SeitenJurnal 2Putri AdnyaniNoch keine Bewertungen
- Spread of Hinduism To South East Asia by Land and Maritime RoutesDokument36 SeitenSpread of Hinduism To South East Asia by Land and Maritime RoutesUday DokrasNoch keine Bewertungen
- S120 Technical Specifications - 23 Dec 21Dokument17 SeitenS120 Technical Specifications - 23 Dec 21jayraj jadejaNoch keine Bewertungen
- Standard MissileDokument2 SeitenStandard Missilemadox_3m100% (1)
- Theory-Set & Relations PDFDokument4 SeitenTheory-Set & Relations PDFmp SinghNoch keine Bewertungen
- MCQ Unit 3Dokument15 SeitenMCQ Unit 3gaur1234Noch keine Bewertungen
- SpiralsDokument12 SeitenSpiralskkglobalNoch keine Bewertungen
- MCA Lab ManualDokument5 SeitenMCA Lab ManualV SATYA KISHORENoch keine Bewertungen
- Dell Inspiron 16 5000 (5625) Laptop - Dell IndiaDokument5 SeitenDell Inspiron 16 5000 (5625) Laptop - Dell IndiamubbunNoch keine Bewertungen
- 7UM512 CatalogueDokument12 Seiten7UM512 Cataloguebuianhtuan1980Noch keine Bewertungen
- Antena Kathrein 742266 PDFDokument2 SeitenAntena Kathrein 742266 PDFcesarbayonaNoch keine Bewertungen
- 447.010 Screen Operating Manual v001Dokument67 Seiten447.010 Screen Operating Manual v001José CarlosNoch keine Bewertungen
- Marxist Study of The God of Small ThingsDokument11 SeitenMarxist Study of The God of Small ThingsIsrar KhanNoch keine Bewertungen
- ABB Photovoltaic DisconnectorsDokument6 SeitenABB Photovoltaic DisconnectorsBog PenNoch keine Bewertungen
- Animal Whisperer PDFDokument4 SeitenAnimal Whisperer PDFKevinPriestmanNoch keine Bewertungen
- Starlift MetricDokument2 SeitenStarlift MetricCralesNoch keine Bewertungen
- ISNGI 2017 ProgrammeDokument6 SeitenISNGI 2017 ProgrammeJoanna JohnsonNoch keine Bewertungen
- Assignment Class X Similar Triangles: A D E B CDokument2 SeitenAssignment Class X Similar Triangles: A D E B CCRPF School100% (1)
- Mechanical Components SectionDokument428 SeitenMechanical Components Sectionxristo xristovNoch keine Bewertungen
- Unipoxy LiningDokument3 SeitenUnipoxy LiningDien Thoai Nguyen HuuNoch keine Bewertungen
- Hirschsprung's Disease - AthigamanDokument128 SeitenHirschsprung's Disease - Athigamanprived100% (4)
- Soul Wars - Wrath of EverchosenDokument107 SeitenSoul Wars - Wrath of EverchosenRyan BelandNoch keine Bewertungen
- Foods 09 01560 PDFDokument10 SeitenFoods 09 01560 PDFkim cheNoch keine Bewertungen
- Examination Speaking Assignments Term III - 2021Dokument2 SeitenExamination Speaking Assignments Term III - 2021Khrystyna ShkilniukNoch keine Bewertungen
- Vol 2 No S12022 Actasdela XVIIConferencia Mundialsobre CineantropometraDokument185 SeitenVol 2 No S12022 Actasdela XVIIConferencia Mundialsobre CineantropometraAye JaimeNoch keine Bewertungen
- Ncs University System Department of Health Sciences: Discipline (MLT-04) (VIROLOGY &MYCOLOGY)Dokument5 SeitenNcs University System Department of Health Sciences: Discipline (MLT-04) (VIROLOGY &MYCOLOGY)Habib UllahNoch keine Bewertungen
- Electrical Inspections: Infrared ThermographyDokument28 SeitenElectrical Inspections: Infrared ThermographyManish RajNoch keine Bewertungen
- Gurps Fallout HandgunsDokument1 SeiteGurps Fallout HandgunsAndrew Scott100% (1)
- Ashok Leyland LimitedDokument19 SeitenAshok Leyland LimitedgsNoch keine Bewertungen
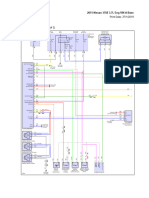
- 2015 Nissan 370Z 3.7L Eng VIN A BaseDokument69 Seiten2015 Nissan 370Z 3.7L Eng VIN A BaseData TécnicaNoch keine Bewertungen