Das könnte Ihnen auch gefallen
- Spinal Cord Injury NCPDokument2 SeitenSpinal Cord Injury NCPShengxy Ferrer100% (6)
- Spinal Cord Injury NCPDokument2 SeitenSpinal Cord Injury NCPEmmanuelRodriguez100% (1)
- Nursing Care Plan - Spinal Cord InjuryDokument2 SeitenNursing Care Plan - Spinal Cord Injuryderic92% (36)
- Spinal Cord InjuryDokument30 SeitenSpinal Cord InjuryKylie Golindang100% (9)
- Nursing Care Plan For Acute Head InjuryDokument4 SeitenNursing Care Plan For Acute Head InjuryAngie Mandeoya67% (3)
- Patho Physiology Spinal Cord InjuryDokument2 SeitenPatho Physiology Spinal Cord InjuryIris Caberte100% (1)
- Spinal Injury Nursing Care PlanDokument2 SeitenSpinal Injury Nursing Care PlanPatricia OrtegaNoch keine Bewertungen
- NCP PainDokument2 SeitenNCP PainKarizza Reyes Mamaradlo100% (1)
- NXCP Disturbed Sensory Perception3Dokument2 SeitenNXCP Disturbed Sensory Perception3marielle_dellaNoch keine Bewertungen
- NCP - Risk Impaired Skin RT Altered Circulation (Spinal Injury)Dokument2 SeitenNCP - Risk Impaired Skin RT Altered Circulation (Spinal Injury)yanny0350% (2)
- Potts Disease NCP .. JustificationDokument8 SeitenPotts Disease NCP .. JustificationMicah SalesNoch keine Bewertungen
- Altered Sensory and Disturbed Thought ProcessDokument4 SeitenAltered Sensory and Disturbed Thought ProcessRosecinie Torrente100% (2)
- NCP - Tissue Perfusion (Cerebral)Dokument2 SeitenNCP - Tissue Perfusion (Cerebral)moodlayers50% (6)
- Nursing Care Plan Format Name: - Medical Diagnosis: Myasthenia Gravis DateDokument2 SeitenNursing Care Plan Format Name: - Medical Diagnosis: Myasthenia Gravis DateSheryl Ann Barit Pedines100% (1)
- Brain TumorDokument9 SeitenBrain TumorKaren Viviene Cinco100% (4)
- Spinal Cord InjuryDokument16 SeitenSpinal Cord Injuryjohnlester_jlf100% (2)
- NCP: FracturesDokument21 SeitenNCP: FracturesJavie100% (1)
- Spinal Cord InjuryDokument26 SeitenSpinal Cord Injurymardsz100% (13)
- Nursing Care Plan For Multiple Sclerosis NCPDokument2 SeitenNursing Care Plan For Multiple Sclerosis NCPderic88% (17)
- Impaired Physical Mobility Related To Neuromuscular ImpairmentDokument17 SeitenImpaired Physical Mobility Related To Neuromuscular ImpairmentAileen Lopez83% (6)
- Pa Tho Physiology of Spinal Cord InjuryDokument1 SeitePa Tho Physiology of Spinal Cord InjuryGenel Joseph Jacildo Peñaflor100% (2)
- Poc Pott's DiseaseDokument8 SeitenPoc Pott's Diseasealsbeth50% (4)
- 14 Cerebrovascular Accident Nursing Care PlansDokument5 Seiten14 Cerebrovascular Accident Nursing Care PlansNickesha Mckenzie75% (4)
- Impaired Physical Mobility RT Neuromuscular Skeletal Impairment.Dokument3 SeitenImpaired Physical Mobility RT Neuromuscular Skeletal Impairment.Abegail Abaygar100% (2)
- Spinal Cord Injury: Causation & PathophysiologyDokument10 SeitenSpinal Cord Injury: Causation & Pathophysiologycpradheep100% (3)
- NCP - Decreased Intracranial Adaptive Capacity R/T Space - Occupying Lesion.Dokument1 SeiteNCP - Decreased Intracranial Adaptive Capacity R/T Space - Occupying Lesion.Carl Elexer Cuyugan Ano100% (6)
- Impaired Verbal CommDokument3 SeitenImpaired Verbal CommKM100% (2)
- Case Study Spinal Cord Injury2Dokument3 SeitenCase Study Spinal Cord Injury2kayevhin0533% (3)
- ThyroidectomyDokument2 SeitenThyroidectomyYenyen Legas100% (2)
- Stroke Nursing Care PlanDokument1 SeiteStroke Nursing Care PlanTracy PearlNoch keine Bewertungen
- Nursing Care Plan - Impaired Physical MobilityDokument2 SeitenNursing Care Plan - Impaired Physical MobilitySusan Croce57% (7)
- NCP AnginaDokument3 SeitenNCP AnginaShie LA100% (1)
- Pathophysiology of Spinal Cord Injury ExplainedDokument5 SeitenPathophysiology of Spinal Cord Injury ExplainedUmar FarooqNoch keine Bewertungen
- CVA Activity IntoleranceDokument1 SeiteCVA Activity IntoleranceNursesLabs.com75% (4)
- Nursing Care Plan: West Visayas State University College of NursingDokument4 SeitenNursing Care Plan: West Visayas State University College of NursingLizaEllaga100% (1)
- Nursing Care Plan (Compartment Sydnrome)Dokument6 SeitenNursing Care Plan (Compartment Sydnrome)Zyiv BalogalNoch keine Bewertungen
- Pathophysiology of CVADokument1 SeitePathophysiology of CVAYoussry JaranillaNoch keine Bewertungen
- Nursing Care Plan For "Herniated Nucleus Pulposus Ruptured Inter Vertebral Disc"Dokument9 SeitenNursing Care Plan For "Herniated Nucleus Pulposus Ruptured Inter Vertebral Disc"jhonroks100% (7)
- NCP Chronic ConfusionDokument4 SeitenNCP Chronic ConfusionLyka DianaNoch keine Bewertungen
- Skin Integrity Nursing Care for ElderlyDokument2 SeitenSkin Integrity Nursing Care for ElderlyRazz Domenique Reyes Escaros100% (5)
- Self Care DeficitDokument3 SeitenSelf Care DeficitAddie Labitad100% (2)
- NCP CvaDokument4 SeitenNCP CvamannyV1990100% (1)
- Mobility Nursing Diagnosis GuideDokument3 SeitenMobility Nursing Diagnosis GuideYan ReyesNoch keine Bewertungen
- Week 10 Drug Card - Hydrochlorothiazide (HCTZ)Dokument2 SeitenWeek 10 Drug Card - Hydrochlorothiazide (HCTZ)RCurry09Noch keine Bewertungen
- NCP LocDokument2 SeitenNCP LocMel RodolfoNoch keine Bewertungen
- NCP - Risk For Peripheral Neurovascular DysfunctionDokument2 SeitenNCP - Risk For Peripheral Neurovascular DysfunctionRene John Francisco50% (4)
- Guillain-Barré Syndrome Autoimmune Attack Peripheral NervesDokument5 SeitenGuillain-Barré Syndrome Autoimmune Attack Peripheral Nervesavinash dhameriyaNoch keine Bewertungen
- Nursing DiagnosisDokument10 SeitenNursing DiagnosisZaty ChaiyOkk100% (1)
- Acute Coronary Syndrome NCP 03Dokument6 SeitenAcute Coronary Syndrome NCP 03AgronaSlaughterNoch keine Bewertungen
- NCPDokument17 SeitenNCPShayne Jessemae AlmarioNoch keine Bewertungen
- Nursing DiagnosisDokument16 SeitenNursing DiagnosisSi Bunga JonquilleNoch keine Bewertungen
- Causes and Nursing Care of Pleural EffusionDokument4 SeitenCauses and Nursing Care of Pleural EffusionHania Polangi100% (1)
- NCP Cardio PrintDokument7 SeitenNCP Cardio PrintNicole MapiliNoch keine Bewertungen
- Guillain - Barre Syndrome (Polyradiculoneuritis)Dokument7 SeitenGuillain - Barre Syndrome (Polyradiculoneuritis)Nadjmiah N. GuilingNoch keine Bewertungen
- Nursing Care Plan: Epidural Hematoma Post CraniotomyDokument14 SeitenNursing Care Plan: Epidural Hematoma Post CraniotomyTepperoni78% (23)
- RAPID SEQUENCE INTUBATION TECHNIQUEDokument55 SeitenRAPID SEQUENCE INTUBATION TECHNIQUElorkan19100% (1)
- Asthma Nursing Care Plan - NCP - Ineffective Airway ClearanceDokument2 SeitenAsthma Nursing Care Plan - NCP - Ineffective Airway ClearanceCyrus De Asis92% (24)
- Ineffective Airway ClearanceDokument2 SeitenIneffective Airway ClearanceHanya Bint PotawanNoch keine Bewertungen
- RehabDokument21 SeitenRehabSalma AfifiNoch keine Bewertungen
- Correos Electrónicos 1-S2.0-S0733861911000879-MainDokument25 SeitenCorreos Electrónicos 1-S2.0-S0733861911000879-Mainjcr87Noch keine Bewertungen
- Cpdprovider Nursing 81718Dokument25 SeitenCpdprovider Nursing 81718PRC BoardNoch keine Bewertungen
- Cpdprogram Nursing 81718Dokument301 SeitenCpdprogram Nursing 81718PRC BoardNoch keine Bewertungen
- Gestational Diabetes Mellitus PathophysiologyDokument1 SeiteGestational Diabetes Mellitus PathophysiologyCyrus De Asis100% (3)
- Major Effects Hormones Pregnant MotherDokument1 SeiteMajor Effects Hormones Pregnant MotherCyrus De AsisNoch keine Bewertungen
- Cerebrovascular Accident Nursing Care PlanDokument4 SeitenCerebrovascular Accident Nursing Care PlanCyrus De Asis67% (12)
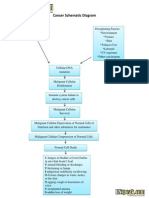
- Cancer Schematic DiagramDokument1 SeiteCancer Schematic DiagramCyrus De Asis100% (4)
- Coronary Artery Disease PathophysiologyDokument4 SeitenCoronary Artery Disease PathophysiologyCyrus De Asis89% (9)
- Schizophrenia Schematic DiagramDokument1 SeiteSchizophrenia Schematic DiagramCyrus De AsisNoch keine Bewertungen
- Asthma Pathophysiology and DiagramDokument1 SeiteAsthma Pathophysiology and DiagramCyrus De Asis100% (1)
- Pregnacy Induced Hypertension PhysiologyDokument1 SeitePregnacy Induced Hypertension PhysiologyCyrus De AsisNoch keine Bewertungen
- Pregnacy Induced Hypertension - PIH - PathophysiologyDokument2 SeitenPregnacy Induced Hypertension - PIH - PathophysiologyCyrus De Asis100% (2)
- Geriatric Assessment Tool An Application of Core - Care and Cure ModelDokument1 SeiteGeriatric Assessment Tool An Application of Core - Care and Cure ModelCyrus De AsisNoch keine Bewertungen
- Liver Pathophysiology and Schematic DiagramDokument1 SeiteLiver Pathophysiology and Schematic DiagramCyrus De Asis100% (4)
- Iron Deficiency Anemia Schematic DiagramDokument2 SeitenIron Deficiency Anemia Schematic DiagramCyrus De Asis83% (12)
- Diarrhea Nursing Care PlanDokument2 SeitenDiarrhea Nursing Care PlanCyrus De Asis87% (119)
- Anaphylactic Shock PathophysiologyDokument1 SeiteAnaphylactic Shock PathophysiologyCyrus De Asis100% (3)
- Ectopic Pregnancy PathophysiologyDokument1 SeiteEctopic Pregnancy PathophysiologyCyrus De Asis100% (2)
- Hypertension Nursing Care PlanDokument2 SeitenHypertension Nursing Care PlanCyrus De Asis92% (13)
- Burns Nursing Care Plan - NCP - Risk For InfectionDokument1 SeiteBurns Nursing Care Plan - NCP - Risk For InfectionCyrus De AsisNoch keine Bewertungen
- Hiatal Hernia Pathophysiology - Schematic DiagramDokument1 SeiteHiatal Hernia Pathophysiology - Schematic DiagramCyrus De Asis100% (1)
- Hyperthyroidism Pathophysiology and Schematic DiagramDokument1 SeiteHyperthyroidism Pathophysiology and Schematic DiagramCyrus De Asis67% (9)
- Congestive Heart Failure Schematic DiagramDokument1 SeiteCongestive Heart Failure Schematic DiagramCyrus De Asis100% (1)
- Nursing Care Plan Patient EndotrachealDokument2 SeitenNursing Care Plan Patient EndotrachealCyrus De Asis67% (6)
- Benign Prostatic Hyperplasia NCPDokument2 SeitenBenign Prostatic Hyperplasia NCPCyrus De Asis100% (2)
- Schematic Diagram of Alcoholic CirrhosisDokument2 SeitenSchematic Diagram of Alcoholic CirrhosisCyrus De Asis0% (1)
- Preeclampsia Pathophysiology and Schematic DiagramDokument1 SeitePreeclampsia Pathophysiology and Schematic DiagramCyrus De Asis80% (10)
- Hydrocephalus PathophysiologyDokument1 SeiteHydrocephalus PathophysiologyCyrus De Asis100% (1)
- Alzheimer's Disease Nursing Care PlanDokument2 SeitenAlzheimer's Disease Nursing Care PlanCyrus De Asis76% (17)
- Post-Throidectomy Nursing Care PlanDokument2 SeitenPost-Throidectomy Nursing Care PlanCyrus De AsisNoch keine Bewertungen
- Folio Biology A+Dokument67 SeitenFolio Biology A+Nina IsmailNoch keine Bewertungen
- Cheat Sheets For Ventilation 5Dokument19 SeitenCheat Sheets For Ventilation 5Syed Shahrul Naz Syed100% (1)
- Acute Respiratory Distress Syndrome (Ards) : Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, Phd. Haneen Alnuaimi, MSNDokument59 SeitenAcute Respiratory Distress Syndrome (Ards) : Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, Phd. Haneen Alnuaimi, MSNAboodsha ShNoch keine Bewertungen
- Exam Code HAAD4Dokument12 SeitenExam Code HAAD4Carmela Marie Eriguel CuetoNoch keine Bewertungen
- Animal Anatomy and Physiology: Figure Q.18Dokument25 SeitenAnimal Anatomy and Physiology: Figure Q.18hager atefNoch keine Bewertungen
- 5.1 OB-Pulmonary Disorders in Pregnancy (Dr. Bautista)Dokument10 Seiten5.1 OB-Pulmonary Disorders in Pregnancy (Dr. Bautista)Monique BorresNoch keine Bewertungen
- ACFrOgDACnKE0rUjf42HXaSb36Wbju Urd7BPPqmTBRXMMFtZ91-fOr1fErSfh6BzXghJFKNYiKG5H-y3ET76l8IkKipRRxFa4B6gSp0OP6njH7C 5ulv8f C1cL DaDokument209 SeitenACFrOgDACnKE0rUjf42HXaSb36Wbju Urd7BPPqmTBRXMMFtZ91-fOr1fErSfh6BzXghJFKNYiKG5H-y3ET76l8IkKipRRxFa4B6gSp0OP6njH7C 5ulv8f C1cL Dajelena_stankovic_34Noch keine Bewertungen
- Original Article: Effects of A Respiratory Physiotherapy Session in Patients With LRTI: A Pre/post-Test StudyDokument10 SeitenOriginal Article: Effects of A Respiratory Physiotherapy Session in Patients With LRTI: A Pre/post-Test StudyEka BagaskaraNoch keine Bewertungen
- Auto-PEEP and Ventilator Modes ExplainedDokument2 SeitenAuto-PEEP and Ventilator Modes ExplainedBharadwaj P KNoch keine Bewertungen
- Mechanical Ventilator Management ProtocolDokument3 SeitenMechanical Ventilator Management ProtocolRick Frea100% (2)
- ICD 10 Codes for Tuberculosis (TB) DiseasesDokument111 SeitenICD 10 Codes for Tuberculosis (TB) DiseasesMarnitaNoch keine Bewertungen
- Teaching Plan CopdDokument11 SeitenTeaching Plan CopdMary Grace AgataNoch keine Bewertungen
- Ground Glass Opacity (GGO) - A Review of The Diferential Diagnosis in The Era of COVID 19 (1) - WatermarkDokument12 SeitenGround Glass Opacity (GGO) - A Review of The Diferential Diagnosis in The Era of COVID 19 (1) - WatermarkMariana Acevedo JimenezNoch keine Bewertungen
- Auto Flow PDFDokument30 SeitenAuto Flow PDFMuhammad Asim RanaNoch keine Bewertungen
- Cebu Doctors' University Intro to RT Program & Rehab SciencesDokument2 SeitenCebu Doctors' University Intro to RT Program & Rehab SciencesMa.Emmagrace JaldonNoch keine Bewertungen
- URTIDokument2 SeitenURTIYogeshRavalNoch keine Bewertungen
- APC Cardio Catalina-1Dokument21 SeitenAPC Cardio Catalina-1Carmelo ScavoneNoch keine Bewertungen
- NCP 106Dokument8 SeitenNCP 106yer tagalajNoch keine Bewertungen
- Acid Base Balance Pathophysiology NursingDokument7 SeitenAcid Base Balance Pathophysiology Nursinggrad_nurse_2015100% (2)
- M256 MSDSDokument26 SeitenM256 MSDSBrian PonderNoch keine Bewertungen
- Human Body Systems VocabularyDokument4 SeitenHuman Body Systems Vocabularyapi-231946379Noch keine Bewertungen
- G05 - Sci - Master Notes - 2019-20Dokument58 SeitenG05 - Sci - Master Notes - 2019-20Veena KumariNoch keine Bewertungen
- KapnografijaDokument9 SeitenKapnografijaMarijana JakobovićNoch keine Bewertungen
- Design and Simulation of Mechanical VentilatorsDokument13 SeitenDesign and Simulation of Mechanical VentilatorsRaghavNoch keine Bewertungen
- Note On Cardiopulmonary Physiotherapy PDFDokument16 SeitenNote On Cardiopulmonary Physiotherapy PDFTsz Kwan CheungNoch keine Bewertungen
- PNEUMONIILEDokument12 SeitenPNEUMONIILELivia Predoi100% (2)
- Respiratory SystemDokument12 SeitenRespiratory SystemTricia CabiliNoch keine Bewertungen
- Sinobronchial SyndromeDokument3 SeitenSinobronchial Syndromemadhumitha srinivasNoch keine Bewertungen
- 3 Infeksi Saluran Pernafasan Akut (ISPA) PediatricsDokument35 Seiten3 Infeksi Saluran Pernafasan Akut (ISPA) PediatricsCharisma Tiara RessyaNoch keine Bewertungen