Das könnte Ihnen auch gefallen
- Presentation On Sales Letter and Agency LetterDokument12 SeitenPresentation On Sales Letter and Agency LetterGautam AnandNoch keine Bewertungen
- Broker Genius Vs NRZ Entertainment/Nathan Zalta Etc.Dokument42 SeitenBroker Genius Vs NRZ Entertainment/Nathan Zalta Etc.Anonymous 9YsE38IjJNoch keine Bewertungen
- Vitamin D3 100 CWSDokument1 SeiteVitamin D3 100 CWSarron_jacklinNoch keine Bewertungen
- New Goverment Grant IAS 20Dokument70 SeitenNew Goverment Grant IAS 20Eshetie Mekonene AmareNoch keine Bewertungen
- NDNCDokument4 SeitenNDNCpogorelovsaNoch keine Bewertungen
- Festivation Inc.: INSC 20263Dokument20 SeitenFestivation Inc.: INSC 20263BISGroupProject100% (1)
- TSS Marketing Proposal 11 2021Dokument4 SeitenTSS Marketing Proposal 11 2021Louisa-johnson EjenavboNoch keine Bewertungen
- A Complete Carpet Installation Business Plan: A Key Part Of How To Start A Carpet & Flooring Installation BusinessVon EverandA Complete Carpet Installation Business Plan: A Key Part Of How To Start A Carpet & Flooring Installation BusinessNoch keine Bewertungen
- Business Interruption: Coverage, Claims, and Recovery, 2nd EditionVon EverandBusiness Interruption: Coverage, Claims, and Recovery, 2nd EditionNoch keine Bewertungen
- Customs and trade acronym definitionsDokument3 SeitenCustoms and trade acronym definitionslavanyakotaNoch keine Bewertungen
- Global Supply Chain Challenges and OpportunitiesDokument45 SeitenGlobal Supply Chain Challenges and OpportunitiesgeorgegeorgeNoch keine Bewertungen
- Approved Sponsorship Letter For Alcoholic SponsorsDokument2 SeitenApproved Sponsorship Letter For Alcoholic SponsorsFelix Raphael MintuNoch keine Bewertungen
- Freight Forwarding Brochure Web PDFDokument21 SeitenFreight Forwarding Brochure Web PDFMaha LakshmiNoch keine Bewertungen
- Non-Disclosure (Confidentiality) AgreementDokument1 SeiteNon-Disclosure (Confidentiality) AgreementEdward CallowNoch keine Bewertungen
- Vitamin D and The Digestive SystemDokument16 SeitenVitamin D and The Digestive Systemsayangnana17Noch keine Bewertungen
- How To Deal With Freight ForwardersDokument45 SeitenHow To Deal With Freight ForwardersaskarqqqqNoch keine Bewertungen
- Competitor AnalysisDokument6 SeitenCompetitor AnalysisOh ChungNoch keine Bewertungen
- First Aid: Statement of AttainmentDokument1 SeiteFirst Aid: Statement of Attainmentapi-534752201Noch keine Bewertungen
- Distribution Management: What Is Industrial Marketing?Dokument4 SeitenDistribution Management: What Is Industrial Marketing?Mehedul Islam SabujNoch keine Bewertungen
- Broker Carrier AgreementDokument1 SeiteBroker Carrier AgreementJessica MartinezNoch keine Bewertungen
- Rio 2016 Customs Freight Manual FinalDokument77 SeitenRio 2016 Customs Freight Manual FinalVicente MirandaNoch keine Bewertungen
- Music BusinessDokument13 SeitenMusic BusinessShaquita S. A. StubbsNoch keine Bewertungen
- Distribution Strategy for Organic Basmati RiceDokument5 SeitenDistribution Strategy for Organic Basmati RiceJoseph MathewNoch keine Bewertungen
- Filmsourcing EPK - Award-Winning Comedy DramaDokument10 SeitenFilmsourcing EPK - Award-Winning Comedy DramaIslahNoch keine Bewertungen
- Broker Carrier Agreement L1Dokument6 SeitenBroker Carrier Agreement L1Diego Alfaro100% (1)
- Cleveland Airport Transportation Service Provides Affordable Luxury RidesDokument24 SeitenCleveland Airport Transportation Service Provides Affordable Luxury RidesJayeshMulchandaniNoch keine Bewertungen
- Pankhuri - Competitor Analysis PDFDokument29 SeitenPankhuri - Competitor Analysis PDFpankhuri89Noch keine Bewertungen
- Agriculture Fruit Farm Business PlanDokument5 SeitenAgriculture Fruit Farm Business PlanAdegboyegaNoch keine Bewertungen
- F&F LetterDokument3 SeitenF&F LetterJaskeerat Singh50% (2)
- Hardness Conversion TableDokument14 SeitenHardness Conversion TableArun KumarNoch keine Bewertungen
- Teal and Blue Geometric Marketing Proposal Proposal-Combined-CombinedDokument39 SeitenTeal and Blue Geometric Marketing Proposal Proposal-Combined-CombinedAbhilasha MeshramNoch keine Bewertungen
- Glossary of International Freight TermsDokument27 SeitenGlossary of International Freight TermsAnand Khisti.100% (4)
- ARS PESTICIDE PROPERTIES DATABASEDokument360 SeitenARS PESTICIDE PROPERTIES DATABASEDaniel Pulido RojasNoch keine Bewertungen
- Carrier Packet WatermarkDokument9 SeitenCarrier Packet Watermarkapi-269523613Noch keine Bewertungen
- American PetroLog, LLC Broker-Carrier Agreement 1-15-16 PDFDokument7 SeitenAmerican PetroLog, LLC Broker-Carrier Agreement 1-15-16 PDFAnonymous rYe0gZWNoch keine Bewertungen
- Roster Project Version 1 September 2014ADR Service Provider - AuthcheckdamDokument154 SeitenRoster Project Version 1 September 2014ADR Service Provider - AuthcheckdamkkNoch keine Bewertungen
- Driver Qualification File: ChecklistDokument12 SeitenDriver Qualification File: ChecklistmartinNoch keine Bewertungen
- Ryse 2Dokument381 SeitenRyse 2Erik Pelton100% (1)
- The Spirit of Chemical SciencesDokument8 SeitenThe Spirit of Chemical SciencesneemadevNoch keine Bewertungen
- 14 Exhibitor Service ManualDokument134 Seiten14 Exhibitor Service ManualAnusionwu Stanley ObinnaNoch keine Bewertungen
- Guidelines Concerning Distribution Systems and Business Practices Under The Antimonopoly ActDokument47 SeitenGuidelines Concerning Distribution Systems and Business Practices Under The Antimonopoly Actvilanova2007Noch keine Bewertungen
- Inventors AgreementDokument4 SeitenInventors AgreementDevin StickellsNoch keine Bewertungen
- Mike Ilitch ObituaryDokument5 SeitenMike Ilitch ObituaryWXYZ-TV Channel 7 DetroitNoch keine Bewertungen
- Rfa Business Plan Template v2 PDFDokument37 SeitenRfa Business Plan Template v2 PDFVickey MehriyaNoch keine Bewertungen
- 3D Dem - Cfd&demDokument12 Seiten3D Dem - Cfd&demShivangi NaikNoch keine Bewertungen
- Crystal Umbrella, Contractor HandbookDokument30 SeitenCrystal Umbrella, Contractor HandbookcrystalumbrellaNoch keine Bewertungen
- Broker-Shipper Agreement PDFDokument4 SeitenBroker-Shipper Agreement PDFemmanuelhood642Noch keine Bewertungen
- Trouble Funk Recording Contract (1984)Dokument19 SeitenTrouble Funk Recording Contract (1984)Christopher S. HarrisonNoch keine Bewertungen
- Fast Lube Program Guide - 2011Dokument7 SeitenFast Lube Program Guide - 2011OilLubeNewsNoch keine Bewertungen
- AbbrDokument45 SeitenAbbrShashidhar KasturiNoch keine Bewertungen
- Patent Attorneys 201213Dokument128 SeitenPatent Attorneys 201213mokilpoNoch keine Bewertungen
- Ocean Freight Shipping Terms PDFDokument11 SeitenOcean Freight Shipping Terms PDFAnonymous kNVhSwNoch keine Bewertungen
- A Utility-Based Framework for Measuring Customer-Based Brand EquityDokument40 SeitenA Utility-Based Framework for Measuring Customer-Based Brand EquityankurkachariNoch keine Bewertungen
- Carrier Contract Packet Cover SheetDokument17 SeitenCarrier Contract Packet Cover SheetJor JisNoch keine Bewertungen
- 78 - Aspen Dental Motion To Dismiss Decision and Order - Cause No.v3:12-Cv-1565 US District Court Syracuse NYDokument27 Seiten78 - Aspen Dental Motion To Dismiss Decision and Order - Cause No.v3:12-Cv-1565 US District Court Syracuse NYDentist The MenaceNoch keine Bewertungen
- Confidentiality Agreement SummaryDokument34 SeitenConfidentiality Agreement SummaryJames Zachary100% (1)
- Hard Summer Music Festival Final DraftDokument5 SeitenHard Summer Music Festival Final DraftValerie TuNoch keine Bewertungen
- Fruit Farming Business PlanDokument20 SeitenFruit Farming Business Plankehabtemaryam bayleyegnNoch keine Bewertungen
- Contractual Agreement SampleDokument5 SeitenContractual Agreement SamplebacusmariavenusNoch keine Bewertungen
- O Praise The Name LsDokument4 SeitenO Praise The Name LschenNoch keine Bewertungen
- Exam Procedures: Steps for Completing a Biochemistry ExamDokument19 SeitenExam Procedures: Steps for Completing a Biochemistry Exampmp123456Noch keine Bewertungen
- Module05 LeasesDokument31 SeitenModule05 LeaseschenNoch keine Bewertungen
- Northern Beacon 2nd Quarter 2015 (1) - 4Dokument1 SeiteNorthern Beacon 2nd Quarter 2015 (1) - 4chenNoch keine Bewertungen
- Question On Human AnatomyDokument13 SeitenQuestion On Human AnatomyAgayatak Sa ManenNoch keine Bewertungen
- Assessment Types of Assessment MethodsDokument3 SeitenAssessment Types of Assessment Methodsadnansensitive5057Noch keine Bewertungen
- Strategies for Maximizing Teacher-Parent CommunicationDokument14 SeitenStrategies for Maximizing Teacher-Parent CommunicationchenNoch keine Bewertungen
- MeaningfulFeedback June2013 PDFDokument20 SeitenMeaningfulFeedback June2013 PDFchenNoch keine Bewertungen
- Assessment MethodsDokument36 SeitenAssessment MethodsArturo GallardoNoch keine Bewertungen
- Bond Application FormDokument1 SeiteBond Application FormchenNoch keine Bewertungen
- Do 043 S2013Dokument4 SeitenDo 043 S2013boodinNoch keine Bewertungen
- RESOLUTION - Docx - Federation AireneDokument2 SeitenRESOLUTION - Docx - Federation AirenechenNoch keine Bewertungen
- Candidate GacusanaMarijul Career Choice 20150601 TestID1222092Dokument2 SeitenCandidate GacusanaMarijul Career Choice 20150601 TestID1222092chenNoch keine Bewertungen
- Kraft Dougherty Teacher Communication JreeDokument44 SeitenKraft Dougherty Teacher Communication Jreebala_devakumarNoch keine Bewertungen
- Admin GacusanaMarijul Career Choice 20150601 TestID1222092Dokument5 SeitenAdmin GacusanaMarijul Career Choice 20150601 TestID1222092chenNoch keine Bewertungen
- Intro To Medical TechnologyDokument2 SeitenIntro To Medical TechnologyAgayatak Sa ManenNoch keine Bewertungen
- MonomersDokument12 SeitenMonomersAgayatak Sa ManenNoch keine Bewertungen
- Swain - Exam III 110314Dokument6 SeitenSwain - Exam III 110314Agayatak Sa ManenNoch keine Bewertungen
- 2001 CHPT 11Dokument24 Seiten2001 CHPT 11chenNoch keine Bewertungen
- Prob 10Dokument9 SeitenProb 10Agayatak Sa ManenNoch keine Bewertungen
- © 2002 Mcgraw-Hill Ryerson Limited. All Rights ReservedDokument36 Seiten© 2002 Mcgraw-Hill Ryerson Limited. All Rights ReservedchenNoch keine Bewertungen
- Ethics & Professional Conduct in AccountingDokument15 SeitenEthics & Professional Conduct in AccountingchenNoch keine Bewertungen
- 2001 CHPT 21Dokument36 Seiten2001 CHPT 21chenNoch keine Bewertungen
- © 2002 Mcgraw-Hill Ryerson Limited. All Rights ReservedDokument24 Seiten© 2002 Mcgraw-Hill Ryerson Limited. All Rights ReservedchenNoch keine Bewertungen
- Portfolio Corporate Communication AuditDokument8 SeitenPortfolio Corporate Communication Auditapi-580088958Noch keine Bewertungen
- 341 BDokument4 Seiten341 BHomero Ruiz Hernandez0% (3)
- Group Assignment: Consumer Buying Behaviour Towards ChipsDokument3 SeitenGroup Assignment: Consumer Buying Behaviour Towards ChipsvikasNoch keine Bewertungen
- Assignment # 4 26 CH 22Dokument6 SeitenAssignment # 4 26 CH 22Ibrahim AbdallahNoch keine Bewertungen
- ESA 7.6 Configuration GuideDokument460 SeitenESA 7.6 Configuration GuideaitelNoch keine Bewertungen
- Rochester MN Unified Development Code (Draft)Dokument442 SeitenRochester MN Unified Development Code (Draft)randyNoch keine Bewertungen
- Chap1 7Dokument292 SeitenChap1 7Zorez ShabkhezNoch keine Bewertungen
- Merging - Scaled - 1D - & - Trying - Different - CLassification - ML - Models - .Ipynb - ColaboratoryDokument16 SeitenMerging - Scaled - 1D - & - Trying - Different - CLassification - ML - Models - .Ipynb - Colaboratorygirishcherry12100% (1)
- MTD Microwave Techniques and Devices TEXTDokument551 SeitenMTD Microwave Techniques and Devices TEXTARAVINDNoch keine Bewertungen
- Construction of Dormitory & Housing compounds in NorochcholaiDokument33 SeitenConstruction of Dormitory & Housing compounds in Norochcholaisaranga100% (1)
- Dse Placement Report PDFDokument78 SeitenDse Placement Report PDFAbhijithKríshñàNoch keine Bewertungen
- 2012 NAPTIN DocumentDokument48 Seiten2012 NAPTIN DocumentbenaikodonNoch keine Bewertungen
- Medhat CVDokument2 SeitenMedhat CVSemsem MakNoch keine Bewertungen
- Appendix 9A: Standard Specifications For Electrical DesignDokument5 SeitenAppendix 9A: Standard Specifications For Electrical Designzaheer ahamedNoch keine Bewertungen
- TSM V5.3 Technical GuideDokument456 SeitenTSM V5.3 Technical GuideparifsNoch keine Bewertungen
- Mosfet PDFDokument13 SeitenMosfet PDFTad-electronics TadelectronicsNoch keine Bewertungen
- Python Lecture PSBCDokument83 SeitenPython Lecture PSBCPedro RodriguezNoch keine Bewertungen
- CCW Armored Composite OMNICABLEDokument2 SeitenCCW Armored Composite OMNICABLELuis DGNoch keine Bewertungen
- Chrysler Corporation: Service Manual Supplement 1998 Grand CherokeeDokument4 SeitenChrysler Corporation: Service Manual Supplement 1998 Grand CherokeeDalton WiseNoch keine Bewertungen
- Keys and Couplings: Definitions and Useful InformationDokument10 SeitenKeys and Couplings: Definitions and Useful InformationRobert Michael CorpusNoch keine Bewertungen
- Panameterics GF 868 Flare Gas Meter PDFDokument8 SeitenPanameterics GF 868 Flare Gas Meter PDFDaniel DamboNoch keine Bewertungen
- EPA - Regulatory Impact AnalysisDokument822 SeitenEPA - Regulatory Impact AnalysisSugarcaneBlogNoch keine Bewertungen
- Constitutional Law of India-II CCSU LL.B. Examination, June 2015 K-2002Dokument3 SeitenConstitutional Law of India-II CCSU LL.B. Examination, June 2015 K-2002Mukesh ShuklaNoch keine Bewertungen
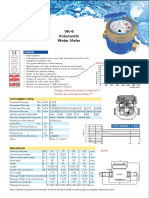
- Baylan: VK-6 Volumetric Water MeterDokument1 SeiteBaylan: VK-6 Volumetric Water MeterSanjeewa ChathurangaNoch keine Bewertungen
- Part 1 - Cutlip and Center's Effective Public Relations. 11th Ed.Dokument127 SeitenPart 1 - Cutlip and Center's Effective Public Relations. 11th Ed.Duyen Pham75% (4)
- 7 - Lakhs Bank EstimateDokument8 Seiten7 - Lakhs Bank Estimatevikram Bargur67% (3)
- ICT FX4Model FrameworkDokument20 SeitenICT FX4Model FrameworkSnowNoch keine Bewertungen
- Nº SSR-1 NS-R-3 Draf R1 Site Evaluation For Nuclear Installations FRDokument33 SeitenNº SSR-1 NS-R-3 Draf R1 Site Evaluation For Nuclear Installations FRdaniel addeNoch keine Bewertungen
- 77115 Maintenance Battery ChargerDokument4 Seiten77115 Maintenance Battery ChargerClarence ClarNoch keine Bewertungen
- Detect Single-Phase Issues with Negative Sequence RelayDokument7 SeitenDetect Single-Phase Issues with Negative Sequence RelayluhusapaNoch keine Bewertungen