Das könnte Ihnen auch gefallen
- Welcome To MEGA PDFDokument9 SeitenWelcome To MEGA PDFRüdiger TischbanNoch keine Bewertungen
- Even More ScaredDokument108 SeitenEven More ScaredManjeev GuragainNoch keine Bewertungen
- SdarticleDokument3 SeitenSdarticleManjeev GuragainNoch keine Bewertungen
- Titanium Framework Removable Partial Denture Used ForDokument4 SeitenTitanium Framework Removable Partial Denture Used ForManjeev GuragainNoch keine Bewertungen
- Child Oral HealthDokument7 SeitenChild Oral HealthManjeev GuragainNoch keine Bewertungen
- Ijms 23 01049Dokument14 SeitenIjms 23 01049Manjeev GuragainNoch keine Bewertungen
- Hypersensitivity To Temporary Soft Denture LinersDokument3 SeitenHypersensitivity To Temporary Soft Denture LinersManjeev GuragainNoch keine Bewertungen
- Sdarticle PDFDokument2 SeitenSdarticle PDFManjeev GuragainNoch keine Bewertungen
- Sdarticle PDFDokument8 SeitenSdarticle PDFManjeev GuragainNoch keine Bewertungen
- Sdarticle PDFDokument4 SeitenSdarticle PDFManjeev GuragainNoch keine Bewertungen
- Sdarticle PDFDokument9 SeitenSdarticle PDFManjeev GuragainNoch keine Bewertungen
- Sdarticle PDFDokument10 SeitenSdarticle PDFManjeev GuragainNoch keine Bewertungen
- Reliability, Validity, and Utility of Various Occlusal Measurement Methods and TechniquesDokument7 SeitenReliability, Validity, and Utility of Various Occlusal Measurement Methods and TechniquesManjeev GuragainNoch keine Bewertungen
- Luzerne Jordan, Washington, D. CDokument2 SeitenLuzerne Jordan, Washington, D. CManjeev GuragainNoch keine Bewertungen
- 12 PDFDokument6 Seiten12 PDFManjeev GuragainNoch keine Bewertungen
- Sdarticle PDFDokument3 SeitenSdarticle PDFManjeev GuragainNoch keine Bewertungen
- Luzerne Jordan, Washington, D. CDokument2 SeitenLuzerne Jordan, Washington, D. CManjeev GuragainNoch keine Bewertungen
- 9 PDFDokument6 Seiten9 PDFManjeev GuragainNoch keine Bewertungen
- 5Dokument9 Seiten5Manjeev GuragainNoch keine Bewertungen
- 8 PDFDokument13 Seiten8 PDFManjeev GuragainNoch keine Bewertungen
- 10 PDFDokument9 Seiten10 PDFManjeev GuragainNoch keine Bewertungen
- President'S Address: Detroit, MichDokument2 SeitenPresident'S Address: Detroit, MichManjeev GuragainNoch keine Bewertungen
- Joel Friedman, Brooklyn, N. Y.: Received 82Dokument5 SeitenJoel Friedman, Brooklyn, N. Y.: Received 82Manjeev GuragainNoch keine Bewertungen
- President'S Address: Detroit, MichDokument2 SeitenPresident'S Address: Detroit, MichManjeev GuragainNoch keine Bewertungen
- 5Dokument9 Seiten5Manjeev GuragainNoch keine Bewertungen
- Dcpavtmelzt of Prosthetics, Ivrrrthsarstcrn Unioersity Dental School, Chicago, 111Dokument3 SeitenDcpavtmelzt of Prosthetics, Ivrrrthsarstcrn Unioersity Dental School, Chicago, 111Manjeev GuragainNoch keine Bewertungen
- Abraham E-I. Lazarus,: New York, N. IDokument5 SeitenAbraham E-I. Lazarus,: New York, N. IManjeev GuragainNoch keine Bewertungen
- DisclaimerDokument2 SeitenDisclaimerManjeev GuragainNoch keine Bewertungen
- Wilfrid Hall Terrell, Calif.: ExaminationDokument25 SeitenWilfrid Hall Terrell, Calif.: ExaminationManjeev GuragainNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Indigenous Women and FeminismDokument27 SeitenIndigenous Women and FeminismClaudia ArteagaNoch keine Bewertungen
- Mgt503 Latest Mcqs Covering Lectures 1 40Dokument79 SeitenMgt503 Latest Mcqs Covering Lectures 1 40prthr100% (1)
- Goethe Elective Affinities TextDokument4 SeitenGoethe Elective Affinities TextAaronNoch keine Bewertungen
- Freedom of SpeechDokument13 SeitenFreedom of SpeechNicolauNoch keine Bewertungen
- ProspectingDokument21 SeitenProspectingCosmina Andreea ManeaNoch keine Bewertungen
- Essential RightDokument42 SeitenEssential Righthamada3747Noch keine Bewertungen
- Semester ReflectionDokument5 SeitenSemester Reflectionapi-316647584Noch keine Bewertungen
- BaZi Basico PDFDokument54 SeitenBaZi Basico PDFMelnicof DanyNoch keine Bewertungen
- Service Marketing Final 29102012Dokument73 SeitenService Marketing Final 29102012Prateek Maheshwari100% (1)
- Ethical Decision Making and Ethical LeadershipDokument11 SeitenEthical Decision Making and Ethical LeadershipmisonotoNoch keine Bewertungen
- Studies in Applied Philosophy, Epistemology and Rational EthicsDokument291 SeitenStudies in Applied Philosophy, Epistemology and Rational EthicsRey Jerly Duran BenitoNoch keine Bewertungen
- ConjunctionDokument2 SeitenConjunctionAngelo Cobacha100% (1)
- He History of ArticulatorsDokument13 SeitenHe History of ArticulatorsrekabiNoch keine Bewertungen
- Fce Speaking Test ChecklistDokument2 SeitenFce Speaking Test Checklist冰泉100% (1)
- AUI4861 Assignment 02 Byron Jason 46433597Dokument18 SeitenAUI4861 Assignment 02 Byron Jason 46433597Byron Jason100% (2)
- Ref Phy 9Dokument1.351 SeitenRef Phy 9mkumar0% (2)
- BRMM 575 Chapter 2Dokument5 SeitenBRMM 575 Chapter 2Moni TafechNoch keine Bewertungen
- Jaimini KarakasDokument3 SeitenJaimini KarakasnmremalaNoch keine Bewertungen
- Trustworthiness and Integrity in Qualitative ResearchDokument25 SeitenTrustworthiness and Integrity in Qualitative ResearchcrossNoch keine Bewertungen
- Category Total Views: 822 This Poetry Has Been Rated 0 Times Rate This PoemDokument2 SeitenCategory Total Views: 822 This Poetry Has Been Rated 0 Times Rate This PoemrajikrajanNoch keine Bewertungen
- 12 Principles in 3D AnimationDokument4 Seiten12 Principles in 3D AnimationfurrypdfNoch keine Bewertungen
- Connections and SymbolsDokument253 SeitenConnections and SymbolsMarko CetrovivcNoch keine Bewertungen
- Darkside Hypnosis - October Man PDFDokument17 SeitenDarkside Hypnosis - October Man PDFManuel Herrera100% (3)
- Upload.c Uhse002 3n12Dokument22 SeitenUpload.c Uhse002 3n12رمزي العونيNoch keine Bewertungen
- Lesson 21 - 30Dokument48 SeitenLesson 21 - 30Rizuanul Arefin EmonNoch keine Bewertungen
- History of ChemistryDokument10 SeitenHistory of ChemistryThamil AnbanNoch keine Bewertungen
- DuBois, The Pan-Africanist and The Development of African Nationalism - Brandon KendhammerDokument22 SeitenDuBois, The Pan-Africanist and The Development of African Nationalism - Brandon KendhammerElmano MadailNoch keine Bewertungen
- Chapter 2013 Multivariate Statistical Analysis IDokument36 SeitenChapter 2013 Multivariate Statistical Analysis IShiera Mae Labial LangeNoch keine Bewertungen
- Kindergarten Science Lesson WormsDokument3 SeitenKindergarten Science Lesson Wormsapi-402679147Noch keine Bewertungen
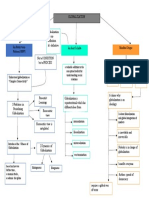
- GCWORLD Concept MapDokument1 SeiteGCWORLD Concept MapMoses Gabriel ValledorNoch keine Bewertungen