Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDokument6 SeitenNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaNoch keine Bewertungen
- Dentin HypersensitivityDokument62 SeitenDentin HypersensitivityVinisha Vipin Sharma100% (1)
- Some Basics of LasersDokument102 SeitenSome Basics of LasersVinisha Vipin SharmaNoch keine Bewertungen
- Pin Retained RestorationDokument31 SeitenPin Retained RestorationVinisha Vipin SharmaNoch keine Bewertungen
- Acupuncture in Dentistry PDFDokument73 SeitenAcupuncture in Dentistry PDFVinisha Vipin SharmaNoch keine Bewertungen
- Minimal Intervention DentistryDokument45 SeitenMinimal Intervention DentistryOmanakuttan KrNoch keine Bewertungen
- 1 Tooth StructureDokument22 Seiten1 Tooth StructurejiwanjyotkaurNoch keine Bewertungen
- Minimal Intervention Dentistry Part 1 - 7 BRITISH DENTAL JOURNAL NOV 10 2012 PDFDokument45 SeitenMinimal Intervention Dentistry Part 1 - 7 BRITISH DENTAL JOURNAL NOV 10 2012 PDFdr parveen bathlaNoch keine Bewertungen
- Ebook - Minimal Intervention DentistrypdfDokument285 SeitenEbook - Minimal Intervention DentistrypdfBerty SusantoNoch keine Bewertungen
- Criteria of SelectionDokument12 SeitenCriteria of SelectionVinisha Vipin SharmaNoch keine Bewertungen
- Diff Betwn Inlay and Amalgam CavityDokument7 SeitenDiff Betwn Inlay and Amalgam CavityVinisha Vipin Sharma100% (1)
- Challenges in Working Length DeterminationDokument101 SeitenChallenges in Working Length DeterminationVinisha Vipin SharmaNoch keine Bewertungen
- Mechanical Preparation Updated May2017 Prof Marco VersianiDokument159 SeitenMechanical Preparation Updated May2017 Prof Marco VersianiVinisha Vipin SharmaNoch keine Bewertungen
- Laser in Conservative Dentistry & EndodonticsDokument75 SeitenLaser in Conservative Dentistry & EndodonticsVinisha Vipin SharmaNoch keine Bewertungen
- Eaat 14 I 1 P 217Dokument6 SeitenEaat 14 I 1 P 217Vinisha Vipin SharmaNoch keine Bewertungen
- Content ServerDokument5 SeitenContent ServerVinisha Vipin SharmaNoch keine Bewertungen
- Content ServerDokument6 SeitenContent ServerVinisha Vipin SharmaNoch keine Bewertungen
- Glide Path PreparationDokument5 SeitenGlide Path PreparationVinisha Vipin SharmaNoch keine Bewertungen
- Show TextDokument1 SeiteShow TextVinisha Vipin SharmaNoch keine Bewertungen
- EchsDokument20 SeitenEchsVinisha Vipin SharmaNoch keine Bewertungen
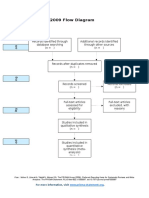
- PRISMA 2009 Flow Diagram: For More Information, VisitDokument1 SeitePRISMA 2009 Flow Diagram: For More Information, VisitVinisha Vipin SharmaNoch keine Bewertungen
- Practice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportDokument5 SeitenPractice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportVinisha Vipin SharmaNoch keine Bewertungen
- Ceramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveDokument5 SeitenCeramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveVinisha Vipin SharmaNoch keine Bewertungen
- Nanodentistry: New Buzz in Dentistry: Review ArticleDokument5 SeitenNanodentistry: New Buzz in Dentistry: Review ArticleVinisha Vipin SharmaNoch keine Bewertungen
- PRISMA-P Statement - Moher Sys Rev Jan 2015Dokument9 SeitenPRISMA-P Statement - Moher Sys Rev Jan 2015Vinisha Vipin SharmaNoch keine Bewertungen
- Clarks Cavity PreparationDokument10 SeitenClarks Cavity PreparationVinisha Vipin SharmaNoch keine Bewertungen
- Esthetic Alternatives To AmalgamDokument15 SeitenEsthetic Alternatives To AmalgamVinisha Vipin SharmaNoch keine Bewertungen
- Klasifikasi GJ Mount and Hume PDFDokument8 SeitenKlasifikasi GJ Mount and Hume PDFlupitaNoch keine Bewertungen
- Minimal Intervention Dentistry: Part 6. Caries Inhibition by Resin InfiltrationDokument8 SeitenMinimal Intervention Dentistry: Part 6. Caries Inhibition by Resin InfiltrationSandra YbarraNoch keine Bewertungen
- Minimal Intervention Dentistry - A Review : FDI Commission Project 1-97Dokument12 SeitenMinimal Intervention Dentistry - A Review : FDI Commission Project 1-97Valeriu IlincaNoch keine Bewertungen
- Dentistry-8-1126 ART 2020Dokument4 SeitenDentistry-8-1126 ART 2020pradnja surya paramithaNoch keine Bewertungen
- Atraumatic Restorative Treatment and Minimal Intervention DentistryDokument7 SeitenAtraumatic Restorative Treatment and Minimal Intervention DentistryKalpanaNoch keine Bewertungen
- Mininmal Intervention DentistryDokument218 SeitenMininmal Intervention DentistryGunjan GargNoch keine Bewertungen
- Introduction To Preventive DentistryDokument4 SeitenIntroduction To Preventive DentistryHaider F YehyaNoch keine Bewertungen