Das könnte Ihnen auch gefallen
- Articulo 2015Dokument2 SeitenArticulo 2015AndreyIvanovNoch keine Bewertungen
- UntitledDokument43 SeitenUntitledJovania B.Noch keine Bewertungen
- Hepatitis B Virus and Liver DiseaseVon EverandHepatitis B Virus and Liver DiseaseJia-Horng KaoNoch keine Bewertungen
- Effects of Vitamin D Supplements in Patients With Chronic Hepatitis C: A Randomized, Multi-Center, Open Label StudyDokument10 SeitenEffects of Vitamin D Supplements in Patients With Chronic Hepatitis C: A Randomized, Multi-Center, Open Label StudyAri Dwi PrasetyoNoch keine Bewertungen
- Keane Et Al-2012-HIV MedicineDokument6 SeitenKeane Et Al-2012-HIV Medicinejulma1306Noch keine Bewertungen
- Study of Liver Cirrhosis Over Ten Consecutive Years in Southern ChinaDokument11 SeitenStudy of Liver Cirrhosis Over Ten Consecutive Years in Southern ChinaDhivya kothandanNoch keine Bewertungen
- Prevalence of Hepatitis B and C Viruses in HIV-positive Patients in China: A Cross-Sectional StudyDokument9 SeitenPrevalence of Hepatitis B and C Viruses in HIV-positive Patients in China: A Cross-Sectional StudyShree Narayan YadavNoch keine Bewertungen
- Hepatitis B Virus - Overview of Management - UpToDateDokument56 SeitenHepatitis B Virus - Overview of Management - UpToDateJoyce SumagaysayNoch keine Bewertungen
- Hepatitis B Virus - Overview of ManagementDokument47 SeitenHepatitis B Virus - Overview of Managementmayteveronica1000Noch keine Bewertungen
- 6009 JFP OnlineExclusiveDokument8 Seiten6009 JFP OnlineExclusiveYAny R SetyawatiNoch keine Bewertungen
- Guideline HBV 2012 UpdateDokument31 SeitenGuideline HBV 2012 UpdateHegandNoch keine Bewertungen
- Role of Hepatitis B Viral Load and Basal Core Promoter Mutation in Hepatocellular Carcinoma in Hepatitis B CarriersDokument8 SeitenRole of Hepatitis B Viral Load and Basal Core Promoter Mutation in Hepatocellular Carcinoma in Hepatitis B CarriersAndrio PalayukanNoch keine Bewertungen
- Guideline of Prevention and Treatment For ChronicDokument22 SeitenGuideline of Prevention and Treatment For ChronicStephania De La CruzNoch keine Bewertungen
- HepeDokument6 SeitenHepegmustafaNoch keine Bewertungen
- A Case of Graves' Disease Accompanied With Acute Hepatitis A Virus InfectionDokument5 SeitenA Case of Graves' Disease Accompanied With Acute Hepatitis A Virus InfectionArini B. MulyaniNoch keine Bewertungen
- 2004 PDFDokument5 Seiten2004 PDFratamanoNoch keine Bewertungen
- Viral Hepatitis (Virus Hepatitis)Dokument66 SeitenViral Hepatitis (Virus Hepatitis)Ilmiah Bagus100% (1)
- Diagnostic Effectiveness of All Test Hbsag Rapid Test Kit Compared With Elisa SerologyDokument3 SeitenDiagnostic Effectiveness of All Test Hbsag Rapid Test Kit Compared With Elisa SerologyHas SimNoch keine Bewertungen
- Zoulim 2014Dokument18 SeitenZoulim 2014Indah LestariNoch keine Bewertungen
- Article 1540976401 PDFDokument3 SeitenArticle 1540976401 PDFnreena aslamNoch keine Bewertungen
- ContentServer - Asp 47Dokument8 SeitenContentServer - Asp 47TataNoch keine Bewertungen
- A Cross-Sectional Study Reagarding Spectrum of Acute Viral Hepatitis at Our HospitalDokument3 SeitenA Cross-Sectional Study Reagarding Spectrum of Acute Viral Hepatitis at Our Hospitalnreena aslamNoch keine Bewertungen
- Journal Reading HIVDokument20 SeitenJournal Reading HIVJeffrey MurphyNoch keine Bewertungen
- 429715457-Serological Markers of Autoimmunity in Children With Hepatitis A, Fulminant PresentaciónDokument9 Seiten429715457-Serological Markers of Autoimmunity in Children With Hepatitis A, Fulminant PresentaciónChristian RosalesNoch keine Bewertungen
- Slide-Diagnosis Dan Interpretasi Hepatitis B KhronikDokument24 SeitenSlide-Diagnosis Dan Interpretasi Hepatitis B KhronikSiti nur rohmahNoch keine Bewertungen
- HaartDokument5 SeitenHaartChikezie OnwukweNoch keine Bewertungen
- Background: Cirrhosis Hepatocellular Carcinoma (HCC)Dokument24 SeitenBackground: Cirrhosis Hepatocellular Carcinoma (HCC)Ignatius Rheza SetiawanNoch keine Bewertungen
- Hepatitis B Virus - Clinical Manifestations and Natural HistoryDokument33 SeitenHepatitis B Virus - Clinical Manifestations and Natural Historymayteveronica1000Noch keine Bewertungen
- Schistosomiasis Case StudyDokument5 SeitenSchistosomiasis Case Studyapi-318749549Noch keine Bewertungen
- Acute HepatitisDokument34 SeitenAcute HepatitisThoma KumaraNoch keine Bewertungen
- HBV Reactivation Risk Factors in Patients With Chronic HBV Infection With Low Replicative State and Resolved HBV Infection Undergoing Hematopoietic Stem Cell Transplantation in KoreaDokument10 SeitenHBV Reactivation Risk Factors in Patients With Chronic HBV Infection With Low Replicative State and Resolved HBV Infection Undergoing Hematopoietic Stem Cell Transplantation in Koreamiss betawiNoch keine Bewertungen
- PatientconferenceM Adadkmnguyen HBV Treatment 06Dokument100 SeitenPatientconferenceM Adadkmnguyen HBV Treatment 06Sakeer PeringodanNoch keine Bewertungen
- Acute Hepatitis E Infection Accounts For Some Cases of Suspected Drug - Induced Liver InjuryDokument17 SeitenAcute Hepatitis E Infection Accounts For Some Cases of Suspected Drug - Induced Liver InjuryBurakkYılmazNoch keine Bewertungen
- Bachelor of Science in Nursing: Ncmb316 Rle: RLE RLE Unit WeekDokument4 SeitenBachelor of Science in Nursing: Ncmb316 Rle: RLE RLE Unit WeekMaica LectanaNoch keine Bewertungen
- Elevation of The Glycated Albumin To Glycated Hemoglobin Atio To Glycated Hemoglobin Atio To Glycated Hemoglobin Atio During The Progression of Hepatitis C Virus Related Liver FibrosisDokument7 SeitenElevation of The Glycated Albumin To Glycated Hemoglobin Atio To Glycated Hemoglobin Atio To Glycated Hemoglobin Atio During The Progression of Hepatitis C Virus Related Liver FibrosistrimardiyanaisyanNoch keine Bewertungen
- Imunosupresie in HCVDokument8 SeitenImunosupresie in HCVdeliaNoch keine Bewertungen
- Hematologic Diseases: High Risk of Associated Diarrhea: Clostridium DifficileDokument7 SeitenHematologic Diseases: High Risk of Associated Diarrhea: Clostridium DifficilePawan MishraNoch keine Bewertungen
- Viral HepatitisDokument20 SeitenViral HepatitisShivam SoniNoch keine Bewertungen
- Long-Term Outcomes of Hbsag/ Anti-Hbs Double-Positive Versus Hbsag Single-Positive Patients With Chronic Hepatitis BDokument7 SeitenLong-Term Outcomes of Hbsag/ Anti-Hbs Double-Positive Versus Hbsag Single-Positive Patients With Chronic Hepatitis BTheresia IlyanNoch keine Bewertungen
- J Bir 2020 10 006Dokument5 SeitenJ Bir 2020 10 006wiam zaimiNoch keine Bewertungen
- Natural History and Clinical Consequences of Hepatitis B Virus InfectionDokument5 SeitenNatural History and Clinical Consequences of Hepatitis B Virus InfectionninacciolyNoch keine Bewertungen
- C, B RecordDokument10 SeitenC, B RecordVjs MrunaliniNoch keine Bewertungen
- Hepatology: Gatot Sugiharto, MD, Internist Faculty of Medicine, UWKS Lecture - 2013Dokument50 SeitenHepatology: Gatot Sugiharto, MD, Internist Faculty of Medicine, UWKS Lecture - 2013niluhayusumbawatiNoch keine Bewertungen
- Jurnal HepatitisDokument5 SeitenJurnal HepatitislevyNoch keine Bewertungen
- HBV Infectionmain Aspects: N. Shavgulidze, MDDokument22 SeitenHBV Infectionmain Aspects: N. Shavgulidze, MDRohan TejaNoch keine Bewertungen
- Tarea s5 Org EspDokument11 SeitenTarea s5 Org EspEduardo EscobarNoch keine Bewertungen
- Chronic Viral HepatitisDokument66 SeitenChronic Viral HepatitisSuresh KadliNoch keine Bewertungen
- Adv in Digestive Medicine - 2020 - Wen - Predictors of HBeAg Loss After Nucleos T Ide Analogues Treatment For ChronicDokument9 SeitenAdv in Digestive Medicine - 2020 - Wen - Predictors of HBeAg Loss After Nucleos T Ide Analogues Treatment For ChronicArushNoch keine Bewertungen
- Unexplained Iron Deficiency Anemia: Does Helicobacter Pylori Have A Role To Play?Dokument6 SeitenUnexplained Iron Deficiency Anemia: Does Helicobacter Pylori Have A Role To Play?dypmcNoch keine Bewertungen
- Anterior Uveitis: A Manifestation of Graft-versus-Host DiseaseDokument4 SeitenAnterior Uveitis: A Manifestation of Graft-versus-Host DiseaseyolandaNoch keine Bewertungen
- Hepatitis A Virus - HAV: DiagnosisDokument6 SeitenHepatitis A Virus - HAV: DiagnosisnurmaliarizkyNoch keine Bewertungen
- Acute Hepatitis: Dr.G.Indhumathi MD.Dokument39 SeitenAcute Hepatitis: Dr.G.Indhumathi MD.Parthiban AnnaduraiNoch keine Bewertungen
- Jurnal Reading 4Dokument29 SeitenJurnal Reading 4Maya SariNoch keine Bewertungen
- Hepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetDokument48 SeitenHepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetNurhidayahNoch keine Bewertungen
- Acute Onset of Autoimmune Hepatitis in Children and Adolescents (PMIDM31474443)Dokument5 SeitenAcute Onset of Autoimmune Hepatitis in Children and Adolescents (PMIDM31474443)yuhonhoNoch keine Bewertungen
- Jaut 1999 0360Dokument5 SeitenJaut 1999 0360Christos ChristidisNoch keine Bewertungen
- CLINPR 100331 Edit ReportDokument8 SeitenCLINPR 100331 Edit Reportjohnysalem88Noch keine Bewertungen
- Incidentally Detected HBsAg Positive SubjectsDokument7 SeitenIncidentally Detected HBsAg Positive SubjectsKhumairaNoch keine Bewertungen
- Gunaid 1997Dokument3 SeitenGunaid 1997Araceli Enríquez OvandoNoch keine Bewertungen
- Case Report: Acute Hepatitis E in A Pediatric Traveler Presenting With Features of Autoimmune Hepatitis: A Diagnostic and Therapeutic ChallengeDokument4 SeitenCase Report: Acute Hepatitis E in A Pediatric Traveler Presenting With Features of Autoimmune Hepatitis: A Diagnostic and Therapeutic Challengeanjingbasah 24Noch keine Bewertungen
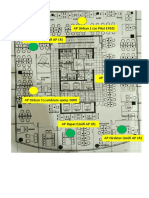
- Topologi Wifi DirbanDokument1 SeiteTopologi Wifi DirbanMaman SulaemanNoch keine Bewertungen
- NIH Public Access: Risk of Waitlist Mortality in Patients With Primary Sclerosing Cholangitis and Bacterial CholangitisDokument16 SeitenNIH Public Access: Risk of Waitlist Mortality in Patients With Primary Sclerosing Cholangitis and Bacterial CholangitisMaman SulaemanNoch keine Bewertungen
- Jsls 14 2 246Dokument5 SeitenJsls 14 2 246Maman SulaemanNoch keine Bewertungen
- Speech Technology: Hearing and Speaking The Google WayDokument1 SeiteSpeech Technology: Hearing and Speaking The Google WayMaman SulaemanNoch keine Bewertungen
- R2868Dokument2 SeitenR2868Maman SulaemanNoch keine Bewertungen
- Mitsubishi IC Pneumatic Forklift PDFDokument5 SeitenMitsubishi IC Pneumatic Forklift PDFfdpc1987Noch keine Bewertungen
- Standard CellDokument53 SeitenStandard CellShwethNoch keine Bewertungen
- Chapter 4Dokument20 SeitenChapter 4Vandan GundaleNoch keine Bewertungen
- Orchid Group of Companies Company ProfileDokument3 SeitenOrchid Group of Companies Company ProfileAngelica Nicole TamayoNoch keine Bewertungen
- Creating A Pathway For Every Student: Holyoke High School Redesign Strategic PlanDokument29 SeitenCreating A Pathway For Every Student: Holyoke High School Redesign Strategic PlanMike PlaisanceNoch keine Bewertungen
- Jean-Louis Cohen - Exhibitionist Revisionism - Exposing Architectural History (September 1999)Dokument10 SeitenJean-Louis Cohen - Exhibitionist Revisionism - Exposing Architectural History (September 1999)Javier PerezNoch keine Bewertungen
- Definite NessDokument398 SeitenDefinite NessKbraNoch keine Bewertungen
- Growth Performance of Papaya Plants As Influenced by Organic MulchesDokument9 SeitenGrowth Performance of Papaya Plants As Influenced by Organic MulchesMa. Christine Lyn AustriaNoch keine Bewertungen
- Eastern Europe SourcebookDokument110 SeitenEastern Europe SourcebookDaniel Alan93% (15)
- Antibiotics and Their Types, Uses, Side EffectsDokument4 SeitenAntibiotics and Their Types, Uses, Side EffectsSpislgal PhilipNoch keine Bewertungen
- Steel Sections PDFDokument36 SeitenSteel Sections PDFTonderai RusereNoch keine Bewertungen
- Operaton Q. PDokument47 SeitenOperaton Q. PPravin KeskarNoch keine Bewertungen
- 3 - RA-Erecting and Dismantling of Scaffolds (WAH) (Recovered)Dokument6 Seiten3 - RA-Erecting and Dismantling of Scaffolds (WAH) (Recovered)hsem Al EimaraNoch keine Bewertungen
- Experiment Number - 1.2 Student Name: Kumar Harsh UID: 21BCS11423 Branch: CSE Section/Group: 508-A Semester: 2 Date of Performance:03/03/2022Dokument4 SeitenExperiment Number - 1.2 Student Name: Kumar Harsh UID: 21BCS11423 Branch: CSE Section/Group: 508-A Semester: 2 Date of Performance:03/03/2022Kartik AgarwalNoch keine Bewertungen
- Triangular Short Crested Weir. Local Geometry ? Discharge CoefficientsDokument7 SeitenTriangular Short Crested Weir. Local Geometry ? Discharge CoefficientsTI Journals PublishingNoch keine Bewertungen
- WCDMA19 Prfile Descriptions W19P8 08A APPRDokument254 SeitenWCDMA19 Prfile Descriptions W19P8 08A APPRoaguilar83Noch keine Bewertungen
- NTCC Project - Fake News and Its Impact On Indian Social Media UsersDokument41 SeitenNTCC Project - Fake News and Its Impact On Indian Social Media UsersManan TrivediNoch keine Bewertungen
- Ponce vs. Court of AppealsDokument7 SeitenPonce vs. Court of AppealsMp CasNoch keine Bewertungen
- Kajima's Three PolicyDokument2 SeitenKajima's Three PolicyBe Seang SeNoch keine Bewertungen
- Internal Audit, Compliance& Ethics and Risk Management: Section 1) 1.1)Dokument6 SeitenInternal Audit, Compliance& Ethics and Risk Management: Section 1) 1.1)Noora Al ShehhiNoch keine Bewertungen
- Performance Management Systems and Strategies by Dipak Kumar BhattacharyyaDokument385 SeitenPerformance Management Systems and Strategies by Dipak Kumar Bhattacharyyasayal96amrit100% (3)
- History of Communication - Project - File - 455 PDFDokument20 SeitenHistory of Communication - Project - File - 455 PDFlathaNoch keine Bewertungen
- Air Defence Systems: Export CatalogueDokument105 SeitenAir Defence Systems: Export CatalogueserrorysNoch keine Bewertungen
- Safe Use of Power Tools Rev0Dokument92 SeitenSafe Use of Power Tools Rev0mohapatrarajNoch keine Bewertungen
- Raw:/storage/emulated/0/download/1623980378472 - 1623980347729 - PE 4 Module 2Dokument11 SeitenRaw:/storage/emulated/0/download/1623980378472 - 1623980347729 - PE 4 Module 2Marvin Espenocilla EspeñoNoch keine Bewertungen
- Nickel 200 201 PDFDokument20 SeitenNickel 200 201 PDFwdavid81Noch keine Bewertungen
- NPN Silicon: Semiconductor Technical DataDokument8 SeitenNPN Silicon: Semiconductor Technical DataMinh Hà QuangNoch keine Bewertungen
- Ecoflam Burners 2014 enDokument60 SeitenEcoflam Burners 2014 enanonimppNoch keine Bewertungen
- Quantum Data-Fitting: PACS Numbers: 03.67.-A, 03.67.ac, 42.50.DvDokument6 SeitenQuantum Data-Fitting: PACS Numbers: 03.67.-A, 03.67.ac, 42.50.Dvohenri100Noch keine Bewertungen