Das könnte Ihnen auch gefallen
- Effect of Cannabis On Human BodyDokument11 SeitenEffect of Cannabis On Human BodySivanu Shifa100% (1)
- Effect of Cannabis On The Human BodyDokument8 SeitenEffect of Cannabis On The Human BodySANDEEP GOUDNoch keine Bewertungen
- Drugs Class 12 ProjectDokument20 SeitenDrugs Class 12 ProjectJitender MorNoch keine Bewertungen
- Biology Investigatory Project: Drug and Alcohol AbuseDokument19 SeitenBiology Investigatory Project: Drug and Alcohol AbuseChomu Dj100% (1)
- QWDokument20 SeitenQWbharad wajNoch keine Bewertungen
- Drug-Addiction-Biology ProjectDokument37 SeitenDrug-Addiction-Biology ProjectAhalya Bai SahooNoch keine Bewertungen
- Investigatory Project Cbse 12thDokument18 SeitenInvestigatory Project Cbse 12thMaheshNoch keine Bewertungen
- Jayen BioDokument16 SeitenJayen BioJayenNoch keine Bewertungen
- Biology Investigatory ProjectDokument19 SeitenBiology Investigatory Projectvaibhav arya100% (1)
- Honey Analysis: A Chemistry Project ReportDokument17 SeitenHoney Analysis: A Chemistry Project ReportSAAIonLINENoch keine Bewertungen
- Bio Investigatory ProjectDokument18 SeitenBio Investigatory ProjectJhilik ChoudhuryNoch keine Bewertungen
- Mar Thoma Higher Secondary School: 2021-2022 CLASS-12 A' Topic - " "Dokument21 SeitenMar Thoma Higher Secondary School: 2021-2022 CLASS-12 A' Topic - " "Sonali JangidNoch keine Bewertungen
- Drug AdiictionDokument17 SeitenDrug AdiictionRahul PatelNoch keine Bewertungen
- Drug Addiction - BIOLOGYDokument37 SeitenDrug Addiction - BIOLOGYamar1972srb81% (149)
- Biology Investigatory ProjectDokument17 SeitenBiology Investigatory ProjectAnonymous CreationsNoch keine Bewertungen
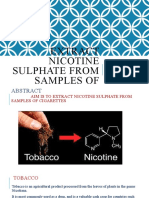
- Extraction of Nicotine From CigarettesDokument5 SeitenExtraction of Nicotine From Cigarettesdiananurallatief0% (1)
- CigaretteDokument25 SeitenCigaretteAmandeep KumarNoch keine Bewertungen
- Project Report On Drugs AddictionDokument5 SeitenProject Report On Drugs AddictionPillarisetty PremsaiNoch keine Bewertungen
- Bio Investigatory ProjectDokument18 SeitenBio Investigatory ProjectJhilik Choudhury100% (3)
- Extract Nicotine Sulphate From Samples of CigaretteDokument11 SeitenExtract Nicotine Sulphate From Samples of CigaretteHema LathaNoch keine Bewertungen
- Analysis of Five Beverages Biology Investigatory Project - Akilesh KumarDokument38 SeitenAnalysis of Five Beverages Biology Investigatory Project - Akilesh KumarTahsheen FarhatNoch keine Bewertungen
- To Detect The Presence of Adulterant (Papaya Seed) in Black Pepper.Dokument11 SeitenTo Detect The Presence of Adulterant (Papaya Seed) in Black Pepper.Kunguma VigneshNoch keine Bewertungen
- Project Report On Drugs AddictionDokument6 SeitenProject Report On Drugs Addictionapi-246586162Noch keine Bewertungen
- Biology Investigatory ProjectDokument38 SeitenBiology Investigatory ProjectHEMAL TUDU100% (1)
- Faridabad: Nav-Jiwan-Public SchoolDokument16 SeitenFaridabad: Nav-Jiwan-Public Schoolsaurabh guptaNoch keine Bewertungen
- Coffee Addiction Biology Investigatory PDokument20 SeitenCoffee Addiction Biology Investigatory PMohit YadavNoch keine Bewertungen
- Chemistry Project On NicotineDokument18 SeitenChemistry Project On NicotineSharun Joshi56% (18)
- Bio Investigatory ProjectDokument16 SeitenBio Investigatory Projectprism1702Noch keine Bewertungen
- Apllication of Biotechnology in MedicineDokument9 SeitenApllication of Biotechnology in MedicineVirendra YadavNoch keine Bewertungen
- Class 12 Biology ProjectDokument15 SeitenClass 12 Biology ProjectARYAN SAJANNoch keine Bewertungen
- Final Class Xii Chem ProjectDokument13 SeitenFinal Class Xii Chem ProjectNITHIN KISHORE NALLATHAMBINoch keine Bewertungen
- Chemistry Investigatory ProjectDokument21 SeitenChemistry Investigatory ProjectSamiha AntaraNoch keine Bewertungen
- Biology Investigatory ProjectDokument21 SeitenBiology Investigatory ProjectSubhiksha100% (1)
- Investigatory Project On: Recombinant DNA Technology in Todays MedicineDokument19 SeitenInvestigatory Project On: Recombinant DNA Technology in Todays MedicineDivyanka Kumari100% (1)
- Drug Addiction Cbse 12th ProjectDokument39 SeitenDrug Addiction Cbse 12th Projecthaneena Riyaz100% (1)
- Chemistry ProjectDokument17 SeitenChemistry ProjectParameswari 1378Noch keine Bewertungen
- Chemistry Investigatory Project On AntacidsDokument13 SeitenChemistry Investigatory Project On AntacidsJoderick Sherwin100% (1)
- Recombinant DNA Technology in Todays MedicineDokument17 SeitenRecombinant DNA Technology in Todays MedicineShailesh100% (1)
- Chemistry Investigatory Project Class 12 Cold DrinkDokument25 SeitenChemistry Investigatory Project Class 12 Cold DrinkZara Hasan0% (1)
- Chemistry ProjectDokument18 SeitenChemistry ProjectAnurup ChattopadhyayNoch keine Bewertungen
- Biology Project To Study BioDokument20 SeitenBiology Project To Study BioRavi Tripathi100% (1)
- Chemistry Investigatory Project On FOOD ADULTERATIONDokument21 SeitenChemistry Investigatory Project On FOOD ADULTERATIONShivansh Tomar63% (8)
- Chemistry Investigatory Project: Detection of Caffeine From Sample of TeaDokument22 SeitenChemistry Investigatory Project: Detection of Caffeine From Sample of TeaKhan Md AribNoch keine Bewertungen
- Shree Swaminarayan Public School Gandhinagar: Chemistry Investigatory ProjectDokument17 SeitenShree Swaminarayan Public School Gandhinagar: Chemistry Investigatory ProjectHoney ModiNoch keine Bewertungen
- Kalyan Chemistry 2Dokument13 SeitenKalyan Chemistry 2Divyanshu PotaliyaNoch keine Bewertungen
- Biology Investigatory Project On Caffeine AddectionDokument5 SeitenBiology Investigatory Project On Caffeine AddectionShivam SinghNoch keine Bewertungen
- Biology Investigatory ProjectDokument9 SeitenBiology Investigatory ProjectSekhar Sahoo54% (13)
- Chemistry Project On Determination of Contents of Cold DrinksDokument11 SeitenChemistry Project On Determination of Contents of Cold Drinksstructure123100% (1)
- Investigatory Project in EnglishDokument13 SeitenInvestigatory Project in EnglishLawl R100% (1)
- Biology Investigatory ProjectDokument21 SeitenBiology Investigatory ProjectAyushi Bisht100% (1)
- Project On: SUBMITTED BY: - SUBMITTED TODokument24 SeitenProject On: SUBMITTED BY: - SUBMITTED TOAayush BhagatNoch keine Bewertungen
- Chromosomes and DNA PackagingDokument15 SeitenChromosomes and DNA PackagingBiju Mylachal100% (1)
- Chemistry Investigatory Project: Xii-O Tagore Public SchoolDokument3 SeitenChemistry Investigatory Project: Xii-O Tagore Public SchoolManish ShuklaNoch keine Bewertungen
- Biology Project File On Drug AddictionDokument9 SeitenBiology Project File On Drug AddictionALIENWARNoch keine Bewertungen
- Chemistry ProjectDokument10 SeitenChemistry ProjectMohd Humair100% (1)
- Chemistry Investigatory ProjectDokument13 SeitenChemistry Investigatory Projectvishlesh parmar100% (1)
- Drug Addiction ProjectDokument22 SeitenDrug Addiction Projectvipoolgetia50% (4)
- Chemistry InvestigatoryDokument10 SeitenChemistry Investigatorypranay shahNoch keine Bewertungen
- Effect of Cannabis On Human BodyDokument11 SeitenEffect of Cannabis On Human Bodyakshatomer43Noch keine Bewertungen
- Review of The Endocannabinoid SystemDokument32 SeitenReview of The Endocannabinoid SystemMoisés Nehémias HernandezNoch keine Bewertungen
- Simple Past TenselDokument3 SeitenSimple Past TenselPutra ViskellaNoch keine Bewertungen
- BIOCHEM REPORT - OdtDokument16 SeitenBIOCHEM REPORT - OdtLingeshwarry JewarethnamNoch keine Bewertungen
- Sample Questions 2019Dokument21 SeitenSample Questions 2019kimwell samson100% (1)
- Trigonometry Primer Problem Set Solns PDFDokument80 SeitenTrigonometry Primer Problem Set Solns PDFderenz30Noch keine Bewertungen
- Jordana Wagner Leadership Inventory Outcome 2Dokument22 SeitenJordana Wagner Leadership Inventory Outcome 2api-664984112Noch keine Bewertungen
- AdvacDokument13 SeitenAdvacAmie Jane MirandaNoch keine Bewertungen
- (Music of The African Diaspora) Robin D. Moore-Music and Revolution - Cultural Change in Socialist Cuba (Music of The African Diaspora) - University of California Press (2006) PDFDokument367 Seiten(Music of The African Diaspora) Robin D. Moore-Music and Revolution - Cultural Change in Socialist Cuba (Music of The African Diaspora) - University of California Press (2006) PDFGabrielNoch keine Bewertungen
- Introduction To Political ScienceDokument18 SeitenIntroduction To Political Sciencecyrene cayananNoch keine Bewertungen
- Layos vs. VillanuevaDokument2 SeitenLayos vs. VillanuevaLaura MangantulaoNoch keine Bewertungen
- Sophia Vyzoviti - Super SurfacesDokument73 SeitenSophia Vyzoviti - Super SurfacesOptickall Rmx100% (1)
- Ib Physics SL - Unit 4 ReviewDokument46 SeitenIb Physics SL - Unit 4 ReviewMax HudgenesNoch keine Bewertungen
- Far Eastern University-Institute of Nursing In-House NursingDokument25 SeitenFar Eastern University-Institute of Nursing In-House Nursingjonasdelacruz1111Noch keine Bewertungen
- S - BlockDokument21 SeitenS - BlockRakshit Gupta100% (2)
- Pilot SafetyDokument120 SeitenPilot SafetyamilaNoch keine Bewertungen
- Capstone Report FormatDokument11 SeitenCapstone Report FormatAnkush PalNoch keine Bewertungen
- Linear Space-State Control Systems Solutions ManualDokument141 SeitenLinear Space-State Control Systems Solutions ManualOrlando Aguilar100% (4)
- Storage Emulated 0 Android Data Com - Cv.docscanner Cache How-China-Engages-South-Asia-Themes-Partners-and-ToolsDokument140 SeitenStorage Emulated 0 Android Data Com - Cv.docscanner Cache How-China-Engages-South-Asia-Themes-Partners-and-Toolsrahul kumarNoch keine Bewertungen
- CogAT 7 PlanningImplemGd v4.1 PDFDokument112 SeitenCogAT 7 PlanningImplemGd v4.1 PDFBahrouniNoch keine Bewertungen
- Favis vs. Mun. of SabanganDokument5 SeitenFavis vs. Mun. of SabanganAyra CadigalNoch keine Bewertungen
- Oldham Rules V3Dokument12 SeitenOldham Rules V3DarthFooNoch keine Bewertungen
- Birds (Aves) Are A Group Of: WingsDokument1 SeiteBirds (Aves) Are A Group Of: WingsGabriel Angelo AbrauNoch keine Bewertungen
- Jurnal Politik Dan Cinta Tanah Air Dalam Perspektif IslamDokument9 SeitenJurnal Politik Dan Cinta Tanah Air Dalam Perspektif Islamalpiantoutina12Noch keine Bewertungen
- Digital Sytems Counters and Registers: Dce DceDokument17 SeitenDigital Sytems Counters and Registers: Dce DcePhan Gia AnhNoch keine Bewertungen
- The Final Bible of Christian SatanismDokument309 SeitenThe Final Bible of Christian SatanismLucifer White100% (1)
- Evaluation of The Agricultural Land Utilization Types For Mitigation of Land Degradation in Giritirta, Pejawaran, BanjarnegaraDokument15 SeitenEvaluation of The Agricultural Land Utilization Types For Mitigation of Land Degradation in Giritirta, Pejawaran, BanjarnegaraTasyaNoch keine Bewertungen
- Action List 50Dokument4 SeitenAction List 50hdfcblgoaNoch keine Bewertungen
- Business Administration: Hints TipsDokument11 SeitenBusiness Administration: Hints Tipsboca ratonNoch keine Bewertungen
- Contracts 2 Special ContractsDokument11 SeitenContracts 2 Special ContractsAbhikaamNoch keine Bewertungen
- A/L 2021 Practice Exam - 13 (Combined Mathematics I) : S.No Name Batch School Ad No. Marks RankDokument12 SeitenA/L 2021 Practice Exam - 13 (Combined Mathematics I) : S.No Name Batch School Ad No. Marks RankElectronNoch keine Bewertungen
- EELE 202 Lab 6 AC Nodal and Mesh Analysis s14Dokument8 SeitenEELE 202 Lab 6 AC Nodal and Mesh Analysis s14Nayr JTNoch keine Bewertungen