Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Movie Star Bodyweight Program GuideDokument14 SeitenMovie Star Bodyweight Program GuideRenzo GottfritNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Exercise Digestive System PDFDokument22 SeitenExercise Digestive System PDFIzudin Hasan86% (7)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- 7... Goldner... Easy Steps To Autoimmune... PBNHC 2015Dokument40 Seiten7... Goldner... Easy Steps To Autoimmune... PBNHC 2015Daniela Constanta Sirbu63% (8)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Chapter 6 Digestion - Lecture NotesDokument9 SeitenChapter 6 Digestion - Lecture Notesapi-372850882% (11)
- Topic 3 Modification of DietsDokument12 SeitenTopic 3 Modification of Dietsmaterwelon ¿Noch keine Bewertungen
- Flavour Dev PDFDokument52 SeitenFlavour Dev PDFBalaji NagendranNoch keine Bewertungen
- Justificacion 7mm MetalDokument5 SeitenJustificacion 7mm MetalMIGUELNoch keine Bewertungen
- Managing Otitis ExternaDokument34 SeitenManaging Otitis ExternaramaNoch keine Bewertungen
- Update in Trauma Anesthesiology Perioperative.12Dokument8 SeitenUpdate in Trauma Anesthesiology Perioperative.12ramaNoch keine Bewertungen
- Managing Otitis ExternaDokument34 SeitenManaging Otitis ExternaramaNoch keine Bewertungen
- Managing Otitis ExternaDokument34 SeitenManaging Otitis ExternaramaNoch keine Bewertungen
- Chole CystitisDokument71 SeitenChole CystitismilarahmaniNoch keine Bewertungen
- Managing Otitis ExternaDokument34 SeitenManaging Otitis ExternaramaNoch keine Bewertungen
- (New) 2. Spine Neuroimaging Dr. BektiDokument42 Seiten(New) 2. Spine Neuroimaging Dr. BektiramaNoch keine Bewertungen
- Oleh: Bagian Ilmu Penyakit Dalam FK Universitas Sultan Agung Semarang 2012Dokument40 SeitenOleh: Bagian Ilmu Penyakit Dalam FK Universitas Sultan Agung Semarang 2012ramaNoch keine Bewertungen
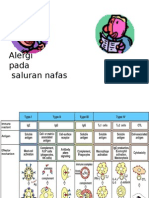
- Alergi Nafas DR - IwangDokument14 SeitenAlergi Nafas DR - IwangramaNoch keine Bewertungen
- Nafld PDFDokument12 SeitenNafld PDFBinaNuraeniNoch keine Bewertungen
- PMK741 0708 A LembaranDokument12 SeitenPMK741 0708 A LembaranramaNoch keine Bewertungen
- Can Non-Alcoholic Fatty Liver Disease (NAFLD) As A Marker For Microalbuminuria in Prediabetes Group?Dokument4 SeitenCan Non-Alcoholic Fatty Liver Disease (NAFLD) As A Marker For Microalbuminuria in Prediabetes Group?BinaNuraeniNoch keine Bewertungen
- Nonalcoholic Fatty Liver - A Possible New Target For Type 2 Diabetes Prevention and Treatment - Ijms-14-22933Dokument34 SeitenNonalcoholic Fatty Liver - A Possible New Target For Type 2 Diabetes Prevention and Treatment - Ijms-14-22933Sanjeev SaxenaNoch keine Bewertungen
- Schreuder, 2008Dokument13 SeitenSchreuder, 2008ramaNoch keine Bewertungen
- Journal of Nutrition College, Volume 1, Nomor 1, Tahun 2012, Halaman 127-133Dokument7 SeitenJournal of Nutrition College, Volume 1, Nomor 1, Tahun 2012, Halaman 127-133ramaNoch keine Bewertungen
- Difference Between Critical and Analytical ThinkingDokument1 SeiteDifference Between Critical and Analytical ThinkingramaNoch keine Bewertungen
- Sartorio PDFDokument7 SeitenSartorio PDFramaNoch keine Bewertungen
- Ko Lester OlDokument25 SeitenKo Lester OlramaNoch keine Bewertungen
- Volume 12, Issue 3, December 2011 - Correlation Between Apolipoprotein B (Apob) Level and Non Alcoholic Fatty Liver in Type 2 Diabetes Mellitus With Metabolic Syndrome PDFDokument4 SeitenVolume 12, Issue 3, December 2011 - Correlation Between Apolipoprotein B (Apob) Level and Non Alcoholic Fatty Liver in Type 2 Diabetes Mellitus With Metabolic Syndrome PDFBriyya LullaniNoch keine Bewertungen
- At 80009Dokument2 SeitenAt 80009Abrian Aziz KNoch keine Bewertungen
- Effect of Food Azo Dyes Tartrazine and Carmoisine On Biochemical ParametersDokument6 SeitenEffect of Food Azo Dyes Tartrazine and Carmoisine On Biochemical ParametersAbdou CherifiNoch keine Bewertungen
- Anti-Nutritional Factors in Some Grain Legumes - A. Mikić, V. Perić, V. Đorđević, M. Srebrić, V. MihailovićDokument8 SeitenAnti-Nutritional Factors in Some Grain Legumes - A. Mikić, V. Perić, V. Đorđević, M. Srebrić, V. MihailovićCk_psihNoch keine Bewertungen
- Health Promotion On Nutrition For Children Under FiveDokument21 SeitenHealth Promotion On Nutrition For Children Under FiveSinta WuLandariNoch keine Bewertungen
- ElvisDokument85 SeitenElvisPaul SimoneNoch keine Bewertungen
- ReportDokument111 SeitenReportrahulprajapNoch keine Bewertungen
- Macronutrient Calculator 1Dokument2 SeitenMacronutrient Calculator 1Andrey CaroNoch keine Bewertungen
- EURRECA Nutritional Planning and Dietary AssessmenDokument6 SeitenEURRECA Nutritional Planning and Dietary AssessmenSonja PavlovicNoch keine Bewertungen
- "Monograph Eating Disorders": StudentDokument12 Seiten"Monograph Eating Disorders": StudentTeffy NeyraNoch keine Bewertungen
- Nutrition EducatorDokument13 SeitenNutrition EducatorDarsan P NairNoch keine Bewertungen
- Anatomija Ljudskog Tijela PDFDokument29 SeitenAnatomija Ljudskog Tijela PDFLejla ImamovićNoch keine Bewertungen
- Nutrition Situation in GujaratDokument13 SeitenNutrition Situation in GujaratDrRameem BlochNoch keine Bewertungen
- Lunch Around The World: by Tracey MiddlekaufDokument10 SeitenLunch Around The World: by Tracey Middlekaufapi-295389842Noch keine Bewertungen
- BMI Baseline Grade SectionDokument8 SeitenBMI Baseline Grade SectionAiza BelandoNoch keine Bewertungen
- Grade 7 Nutrition Month Quiz BowlDokument3 SeitenGrade 7 Nutrition Month Quiz BowlTrisha RequintelNoch keine Bewertungen
- Nourishing CoconutDokument8 SeitenNourishing CoconutNazihCosmeticsNoch keine Bewertungen
- Renal Physiology ch25Dokument19 SeitenRenal Physiology ch25v-santNoch keine Bewertungen
- Latest 2019 ESC Guidelines On DyslipidemiaDokument11 SeitenLatest 2019 ESC Guidelines On DyslipidemiarkNoch keine Bewertungen
- Healthy Dessert Recipes - EnglishDokument10 SeitenHealthy Dessert Recipes - EnglishlwccfilesNoch keine Bewertungen
- Conditioning ProgramDokument4 SeitenConditioning ProgramKiko de la CruzNoch keine Bewertungen
- Production Method For Some Insect Based Food For Local Consumption in Ondo State NigeriaDokument3 SeitenProduction Method For Some Insect Based Food For Local Consumption in Ondo State NigeriaIJARP PublicationsNoch keine Bewertungen
- LTC NCPDokument2 SeitenLTC NCPapi-302841502Noch keine Bewertungen
- Line Graph SamplesDokument14 SeitenLine Graph SamplesThanh Trâm NguyễnNoch keine Bewertungen